
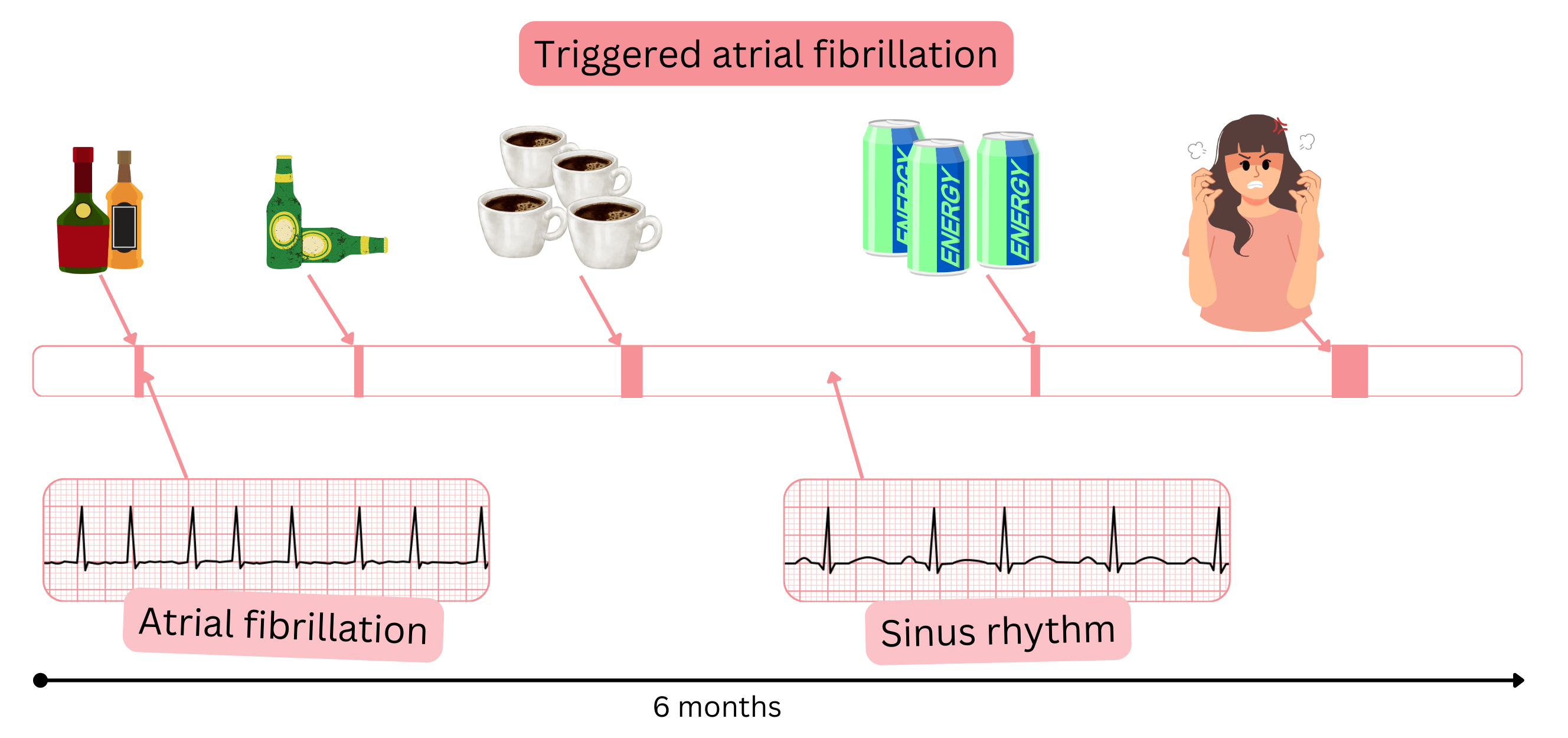
Triggered atrial fibrillation (AF) means that the AF episode has a clear trigger.
The most common AF triggers include an acute critical or high-risk condition.
Sepsis causes AF in up to 20–46% of patients who have not had AF before.
Acute critical condition
| Acute critical condition and incidence of atrial fibrillation (AF) | |
|---|---|
| Acute critical condition | Incidence of AF (%) |
| Cardiac surgery | 30 – 60 % |
| Acute heart failure | 25 – 50 % |
| Sepsis | 20 – 46 % |
| Acute respiratory distress syndrome (ARDS) | 20 – 40 % |
| Stroke | 10 – 30 % |
| Myocardial infarction (STEMI / NSTEMI) | 10 – 22 % |
| Patients in ICU | 5 – 25 % |
| Pulmonary embolism | 5 – 15 % |
| Major bleeding | 3 – 5 % |
Acute high-risk condition
| Acute high-risk condition and incidence of atrial fibrillation (AF) | |
|---|---|
| Acute high-risk condition | Incidence of AF (%) |
| Alcohol excess | 20 – 30 % |
| Drug use (cocaine, methamphetamine, ecstasy) | 5 – 15 % |
| Extreme physical exertion | 2 – 4 % |
| Extreme stress | 2 – 4 % |
| Excessive sun exposure | 1 – 3 % |
| Coffee excess | 1 – 2 % |
| Energy drink excess | 1 – 2 % |
| Drug use (marijuana) | 1 – 2 % |
In clinical practice, however, it usually does not apply that removing the trigger will eliminate AF.
Triggered AF with episodes occurring only after a known trigger is very rare.
If we unequivocally confirm triggered AF in a patient based on a loop recorder,
Treatment of triggered AF is elimination of the trigger (if possible) and management according to the SKC algorithm.
Triggered and “standard” AF have the same risk of thromboembolism.
Anticoagulation therapy in triggered AF is indicated according to the CHA2DS2-VA score.
| Triggered atrial fibrillation | Class |
|---|---|
| In triggered AF, anticoagulation therapy is indicated according to the CHA2DS2-VA score. | I |
| If triggered AF is suspected, an ECG should be recorded during symptoms using an ECG smart device (ECG watch, blood pressure monitor with ECG, ECG card). | IIa |
| Discontinuation of anticoagulation therapy may be considered if a clear trigger has been eliminated (alcohol excess, sepsis, stress, energy drinks). | IIb |
| Implantation of a loop recorder may be considered to definitively confirm triggered AF. | IIb |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
