Terminology of Atrial Fibrillation
Atrial fibrillation (AF) in clinical practice is most commonly classified according to episodes and valvular disease as:
- Newly diagnosed AF (date of first documented AF on ECG)
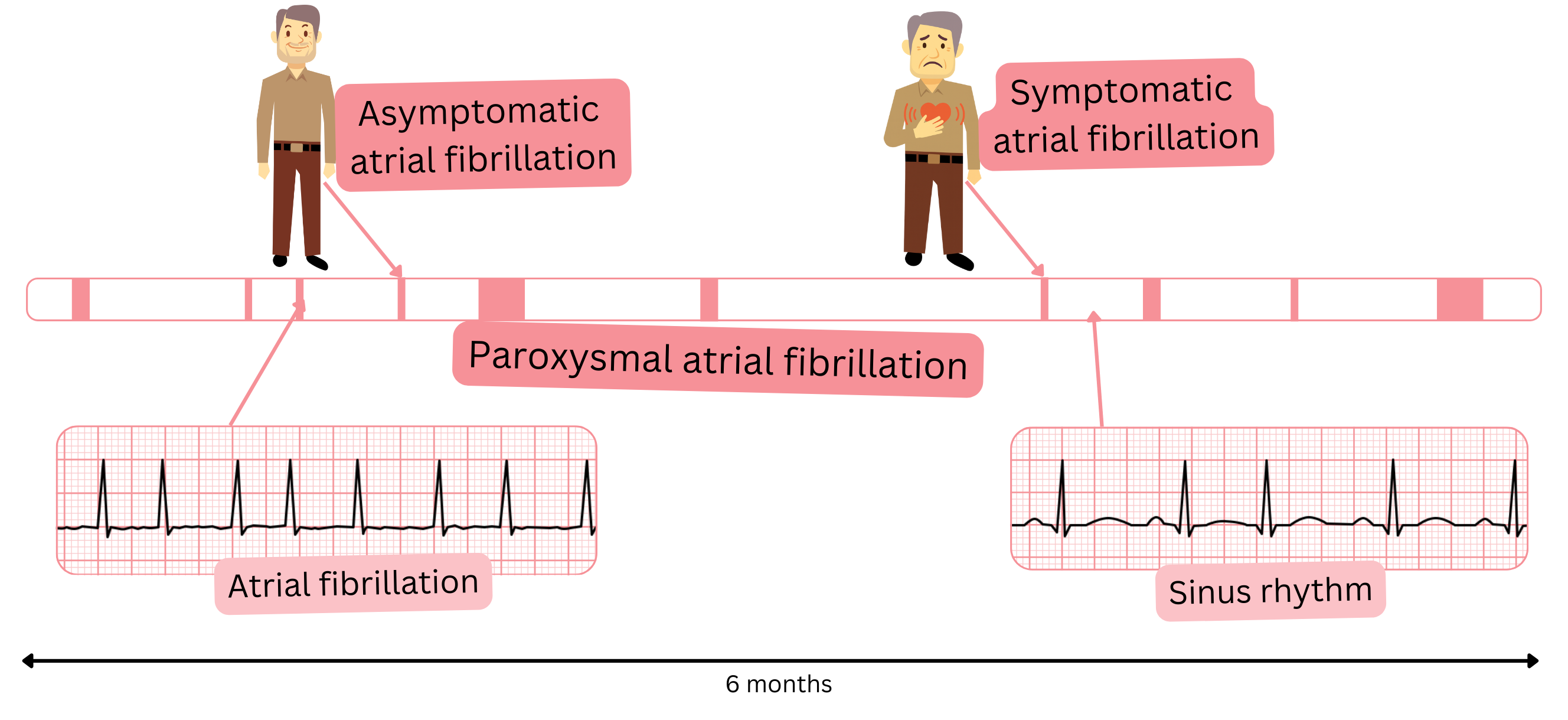
- Paroxysmal AF
- Persistent AF
- Permanent AF
- Valvular AF (mechanical valve or mitral stenosis – moderate or severe)
In clinical practice and in publications, additional terms related to AF are also used. The following table summarizes terminology commonly used in relation to AF.
| Terminology of Atrial Fibrillation According to Clinical Context |
| Clinical AF |
- AF documented on ECG, regardless of whether the patient is symptomatic or asymptomatic.
- Simply put, the patient has AF recorded on ECG.
|
| Asymptomatic AF |
- The patient has clinical AF documented on ECG but does not report any symptoms suggestive of AF.
- In other words, AF is documented on ECG, but the patient does not subjectively perceive it.
|
| Silent AF |
- “Silent” refers to “silent” AF.
- The patient has AF but is unaware of it because it is asymptomatic and has never been captured on ECG.
- It is dangerous because the patient receives no treatment for AF and is at risk of stroke.
- Silent AF occurs in approximately 10 % of patients.
|
| Oligosymptomatic AF |
- “Oligo” in medicine means “few or infrequent symptoms.”
- The patient has mild or non-specific symptoms (fatigue, weakness, reduced exercise tolerance).
- AF may be documented on ECG – the patient knows they have AF.
- or it is not documented on ECG – the patient is unaware they have AF.
- Oligosymptomatic AF not documented on ECG (the patient is unaware of having AF) is dangerous, similar to silent AF, because the patient receives no treatment and is at risk of stroke.
|
| Occult AF |
- “Occult” in medicine means “hidden.”
- The term occult AF is most commonly used in the context of cryptogenic stroke; “cryptogenic” means of unclear origin.
- If a patient experiences a cryptogenic stroke, the most likely cause is silent AF.
- Targeted diagnostic evaluation for AF is then initiated.
- If AF is subsequently confirmed in the context of a cryptogenic stroke, it is referred to as occult AF.
|
| Lone AF |
- Lone AF refers to “isolated AF.”
- AF in a patient without risk factors:
- Age <60 years and
- CHA2DS2-VA score = 0
|
| Tachycardia-induced cardiomyopathy |
- If a patient has AF, particularly persistent or permanent AF, over several months to years there may be:
- cardiac dilatation (especially of the left atrium and ventricle) and
- reduced ejection fraction <40 %
- This cardiac dilatation is reversible; if AF is eliminated, cardiac dimensions improve within approximately 3 months.
- This cardiomyopathy may also occur with other persistent or permanent arrhythmias (atrial flutter, atrial tachycardia).
|
| Tachy AF |
- AF with a ventricular rate >100/min.
- At AF rates >150/min, haemodynamic instability frequently occurs.
|
| Terminology of Atrial Fibrillation According to Duration and Onset |
| New-onset AF |
- AF in which, based on symptoms, we assume duration <24 hours. For example, a patient presents to the clinic because palpitations began 5 hours ago.
- However, it is never possible to know with 100 % certainty that AF has lasted <24 hours, as the patient may have had asymptomatic episodes for months (silent AF).
- The term is used in the context of cardioversion (electrical or pharmacological) to sinus rhythm.
- If AF duration is <24 hours, cardioversion may be performed without significant thromboembolic risk.
- Nevertheless, this can never be known with absolute certainty.
|
| Early AF |
- Early AF refers to “recently diagnosed AF.”
- AF lasting <1 year.
- It may be paroxysmal or persistent.
|
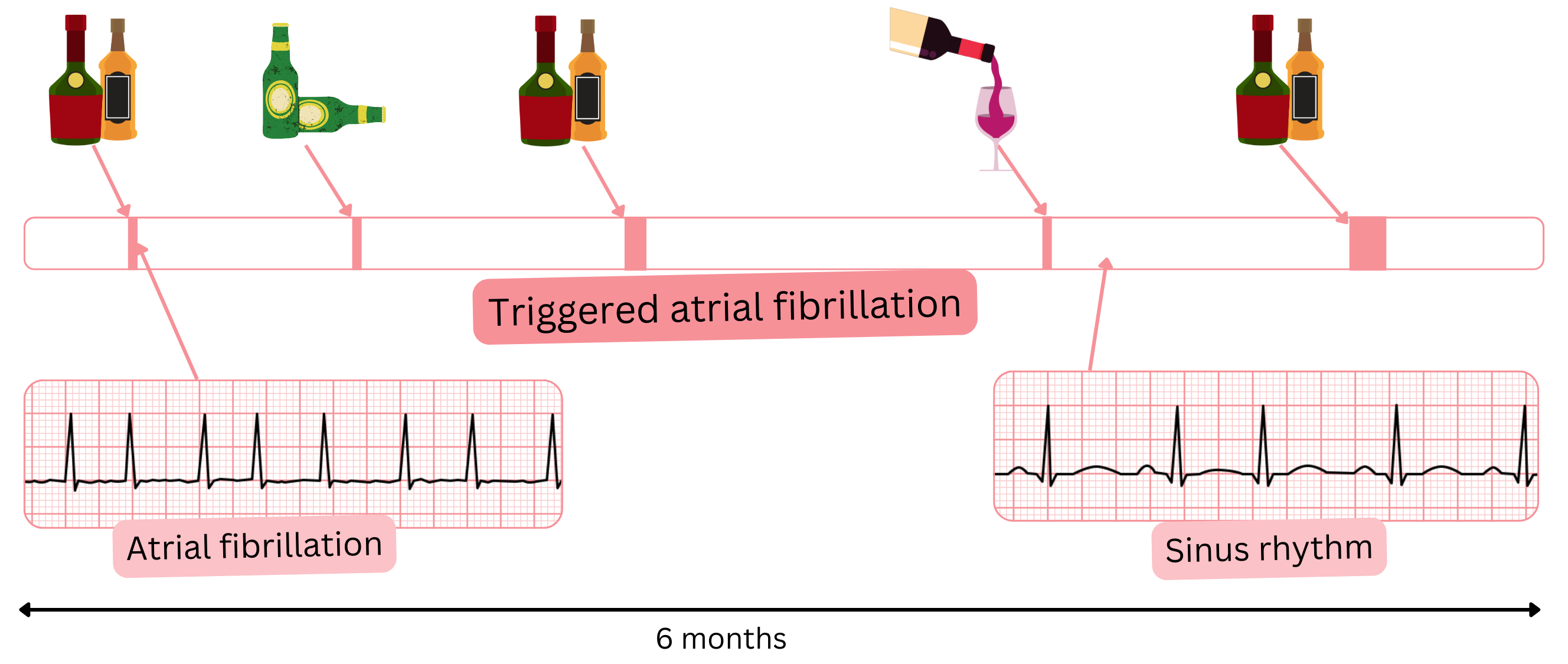
| Triggered AF |
- AF occurring after a clear, identifiable trigger, e.g. alcohol, coffee, energy drinks, stress.
- If the trigger is eliminated, most AF episodes resolve.
|
| Spontaneously terminating AF |
- An AF episode terminates spontaneously, usually within 48 hours.
- The patient may or may not be on chronic pharmacological therapy.
- Most commonly paroxysmal AF.
- Sometimes referred to as intermittent AF.
|
| Intermittent AF |
- Refers to spontaneously terminating AF.
- The term is used very rarely.
|
| Non–spontaneously terminating AF |
- AF that does not terminate spontaneously.
- Usually lasts >7 days.
- Intervention is required for termination (pharmacological or electrical cardioversion).
|
| AF burden |
- “Burden” refers to the AF load.
- It represents the percentage of time spent in AF over a defined period.
- Most commonly assessed using 24-hour Holter ECG or implanted devices (loop recorder, pacemaker).
- For example: On a 24-hour Holter recording, a patient has sinus rhythm and paroxysms of AF totalling 5 hours. AF burden is therefore approximately 20 %.
- AF burden is assessed more precisely with implanted devices, which continuously record cardiac electrical activity, for example over 3 months.
|
In clinical practice and in publications, the following terms are often used:
- AHRE
- Device-detected AHRE
- Subclinical AF
- All three terms are synonyms and mean the same.
| Terminology of Atrial Fibrillation and CIED (Cardiac Implantable Electronic Devices) |
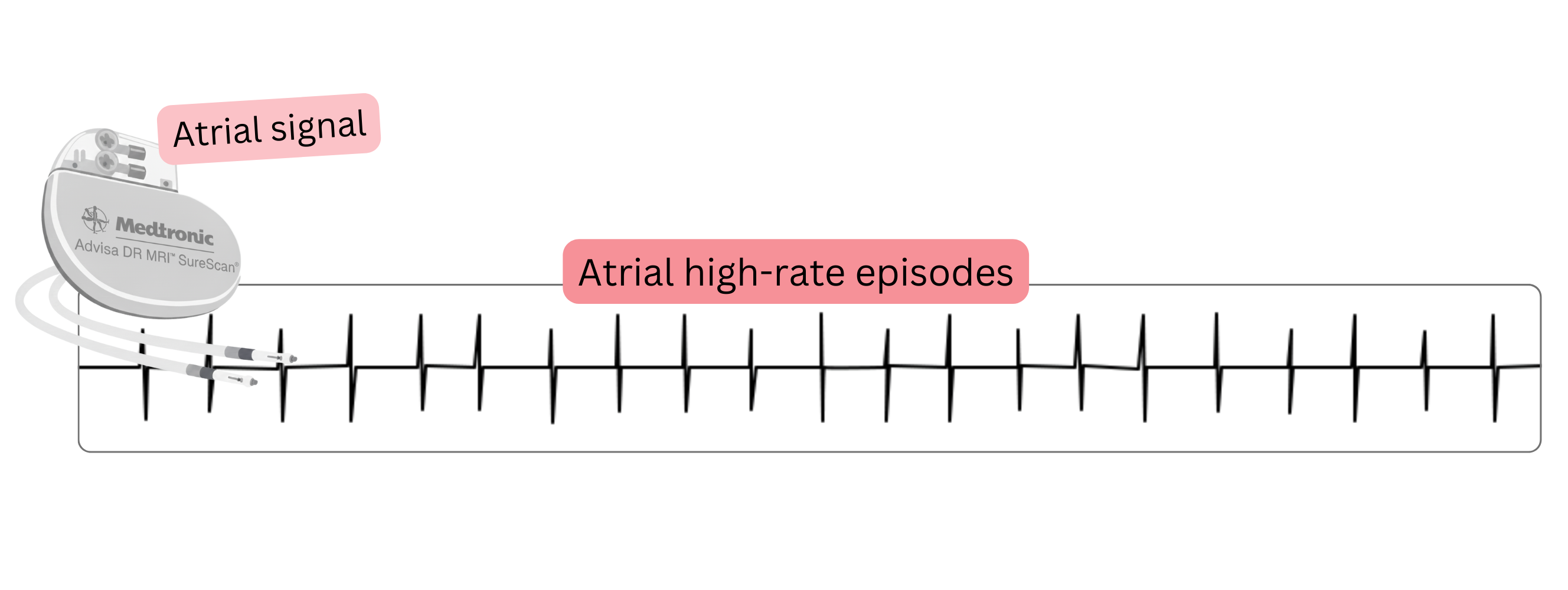
AHRE
(Atrial High Rate Episodes) |
- An episode of atrial tachyarrhythmia lasting >5 min with a rate >170/min.
- Diagnosed using CIED (Cardiac Implantable Electronic Devices) equipped with an atrial lead that senses atrial electrical activity (this is not a surface ECG). These devices include:
- Pacemaker (PCM)
- Defibrillator (ICD)
- Cardiac resynchronization therapy device (CRT)
- Using an atrial lead, these devices detect only high atrial rates; however, their discriminatory capability is lower than that of a surface ECG.
AHRE may represent:
- atrial tachycardia
- atrial flutter
- atrial fibrillation
|
| Device-detected AHRE |
- AHRE is sometimes referred to as device-detected AHRE because it can be detected only by implantable devices (PCM, ICD, CRT).
- Device-detected AHRE is sometimes incorrectly labelled as device-detected AF, as it does not necessarily represent AF.
|
| Subclinical AF |
- Subclinical AF means that “it is likely AF.”
- Clinical AF means that AF is definitively confirmed because it is documented on ECG.
- It refers to an AHRE episode detected by a CIED.
- AHRE does not necessarily represent AF; it may be atrial tachycardia or atrial flutter.
- If no ECG documentation is available during AHRE, the episode cannot be definitively diagnosed as AF.
|
- In clinical practice, there is no uniform agreement regarding AF terminology; therefore, some terms are used interchangeably. The most commonly confused terms are:
- Asymptomatic AF – Silent AF – Occult AF
- Subclinical AF – AHRE – Device-detected AHRE – Occult AF
- Paroxysmal AF – Spontaneously terminating AF – Intermittent AF
- Persistent AF – Non–spontaneously terminating AF
| Terminology of Atrial Fibrillation in Clinical Practice |
Class |
|
The most commonly used AF terminology in clinical practice:
- Clinical AF
- Subclinical AF (AHRE)
- Asymptomatic AF
- Silent AF
- New-onset AF
- Triggered AF
- AF burden
- Tachycardia-induced cardiomyopathy
|
I |
In practice, the highest-risk patients are those with silent AF. These patients have no specific symptoms suggestive of AF.
Patients with silent AF are not receiving anticoagulation therapy and may develop an ischaemic stroke. Stroke risk can be calculated using the CHA2DS2-VA score.

