
Classification:
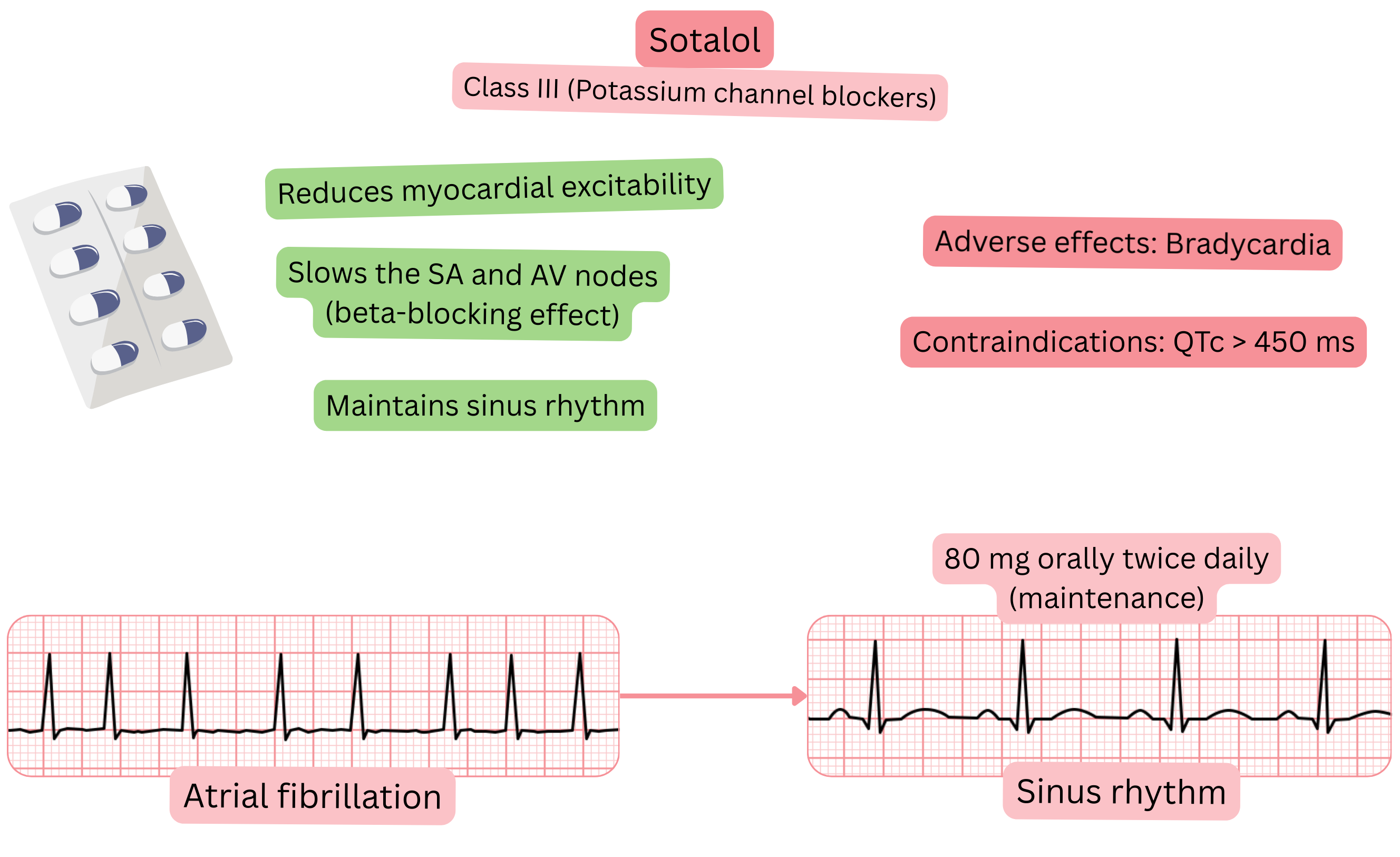
Mechanism:
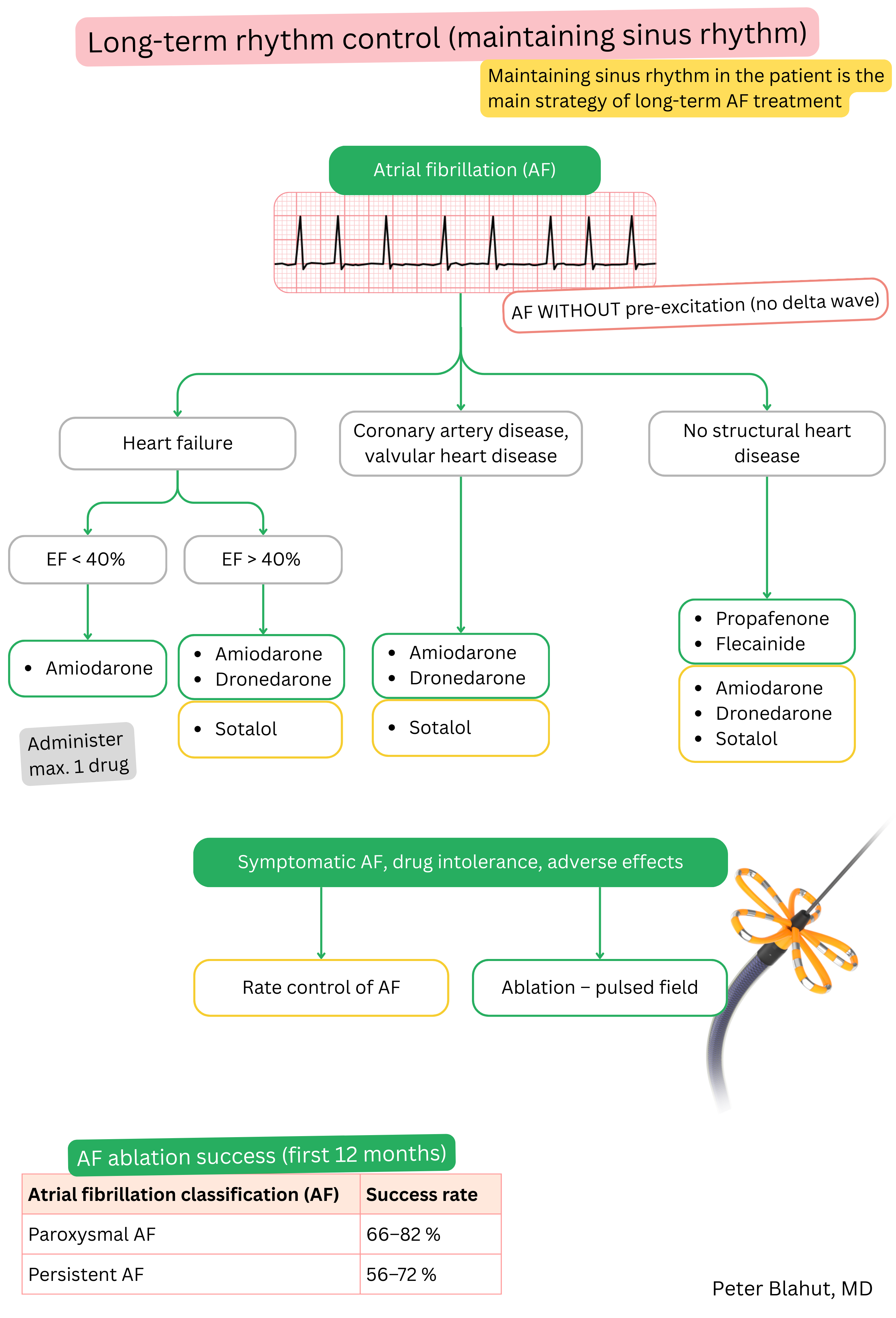
Effect on AF:
| Sotalol and atrial fibrillation (AF) |
|---|
| Brand names |
| Sotalol, Sotalex, Sotacor |
| Indications |
|
| Dosing |
|
| Onset of action |
|
| Effect |
Maintenance of sinus rhythm (paroxysmal or persistent AF) at 1 year
|
| Duration of action |
|
| Contraindications |
|
Patient monitoring after initiation of sotalol:
| Patient monitoring after initiation of sotalol | ||
|---|---|---|
| Time from initiation | What to monitor | Reason for treatment discontinuation |
| 1–3 days (from initiation or after dose increase) |
ECG (QTc) Blood pressure |
QTc > 500 ms Bradycardia < 50/min Hypotension < 90/60 mmHg |
| 7 days – 1 month |
ECG (QTc) Blood pressure Laboratory tests (electrolytes, renal function) |
QTc > 500 ms Bradycardia < 50/min Hypotension < 90/60 mmHg Severe electrolyte imbalance (Na⁺, K⁺, Mg²⁺) |
| 6–12 months |
ECG (QTc) Echocardiography Laboratory tests (electrolytes, renal function) |
QTc > 500 ms Severe electrolyte imbalance (Na⁺, K⁺, Mg²⁺) |
Adverse effects:
| Sotalol vs. beta-blockers in atrial fibrillation (AF) | ||
|---|---|---|
| Property | Sotalol | Beta-blockers |
| Class | Class III + non-selective beta-blocker | Class II (pure beta-blockers) |
| Mechanism | K⁺ channel blockade + β-receptor blockade | β₁ blockade (reduction of heart rate and AV conduction) |
| Effect on QT interval | Prolongs QT (risk of TdP) | No effect on QT |
| Reverse use-dependence | Strong effect at HR < 60/min Weak effect at HR > 100/min |
No |
| Dose dependence |
< 160 mg/day → beta-blocker effect ≥ 160–320 mg/day → beta-blocker + Class III effect |
Dose determines strength of beta-blocker effect, without Class III activity |
| Indication in AF | Maintenance of sinus rhythm (rhythm control) | Heart rate control |
| Adverse effects | Torsades de pointes (at QTc ≥ 500 ms) | Bronchospasm, fatigue, bradycardia, hypotension |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
