
Classification:

Mechanism:
Effect on AF:
| Procainamide and atrial fibrillation (AF) |
|---|
| Brand names |
| Procainamid, Pronestyl, Procan, Procanbid, Novocainamid, Novocamid |
| Indications |
|
| Dosing |
|
| Onset of action |
|
| Effect |
Time to conversion to sinus rhythm and success rate
|
| Duration of action |
|
| Contraindications |
|
Patient monitoring during procainamide administration:
| Patient monitoring during procainamide administration | ||
|---|---|---|
| Monitoring period | What to monitor | Reason for discontinuation |
| During infusion |
ECG (QRS, QTc interval, rhythm) Blood pressure Clinical status (dizziness, weakness) |
QRS widening > 25% QTc > 500 ms Bradycardia < 40/min Hypotension < 90/60 mmHg Ventricular arrhythmia |
| 30–120 minutes after administration |
ECG (QRS, QTc interval, rhythm) Blood pressure Clinical status (dizziness, weakness) |
QRS widening > 25% QTc > 500 ms Bradycardia < 40/min Hypotension < 90/60 mmHg Ventricular arrhythmia |
Adverse effects:
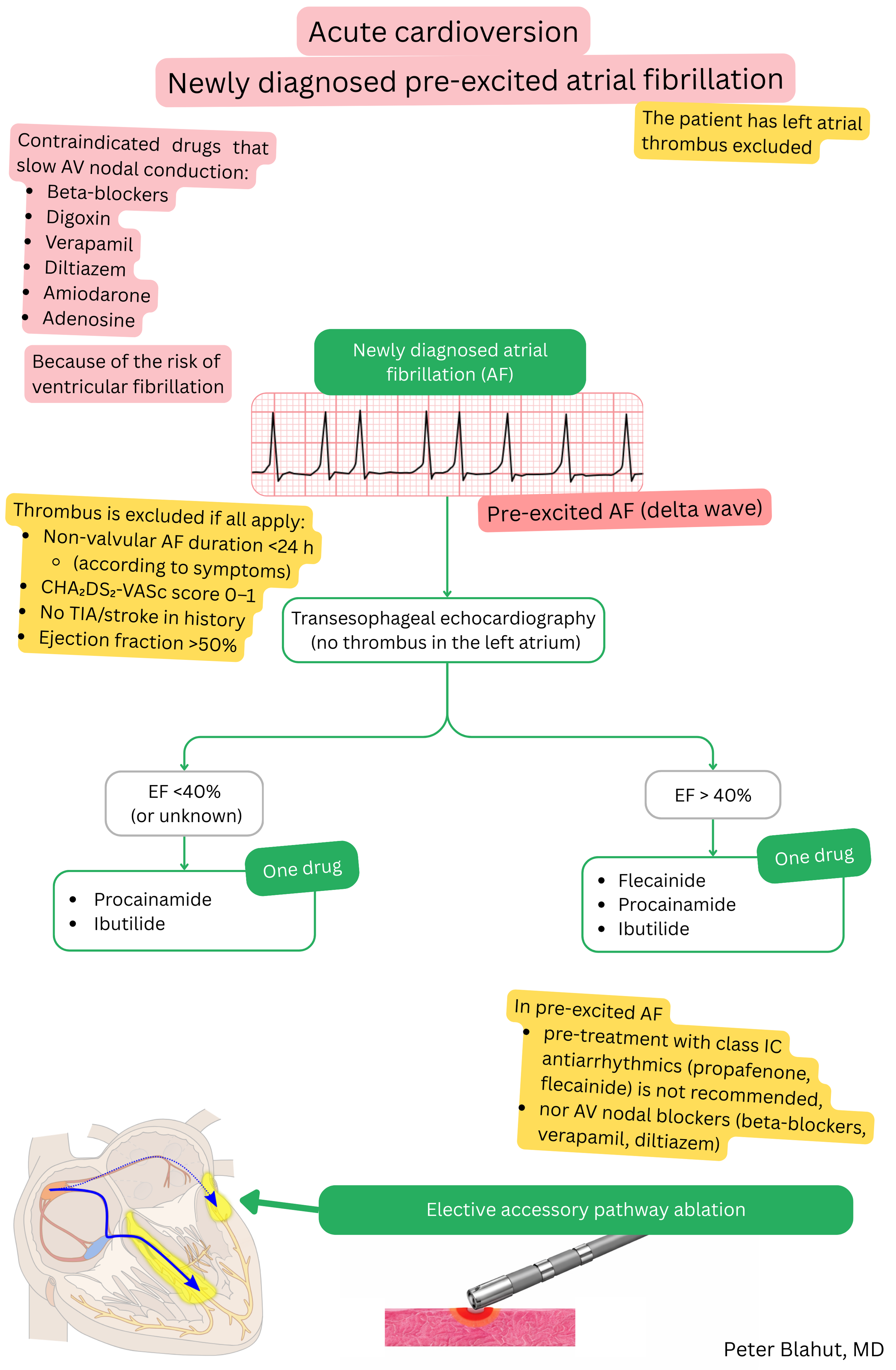
For pharmacological cardioversion of pre-excited AF, both procainamide and ibutilide may be used.
| Procainamide vs Ibutilide and atrial fibrillation | ||
|---|---|---|
| Property | Procainamide | Ibutilide |
| Class | IA (Na⁺ channel blocker, minimal K⁺ blockade) | III (K⁺ channel blocker) |
| Cardioversion of pre-excited AF | Yes – first-line drug | Yes – possible, but less preferred |
| Indication in AF | Acute cardioversion of pre-excited AF | Acute cardioversion of AF or atrial flutter |
| Conversion success rate to SR | 50–75 % (within 30 minutes) | ~30–50 % in AF, 60–75 % in atrial flutter |
| Use in atrial flutter | No | Yes |
| Main risks | Hypotension, proarrhythmia (torsades de pointes), lupus-like syndrome | QT prolongation, torsades de pointes |
| Typical patient | Younger patient with AF and WPW (delta wave on ECG) | Patient with AF or atrial flutter without WPW, for urgent conversion |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
