
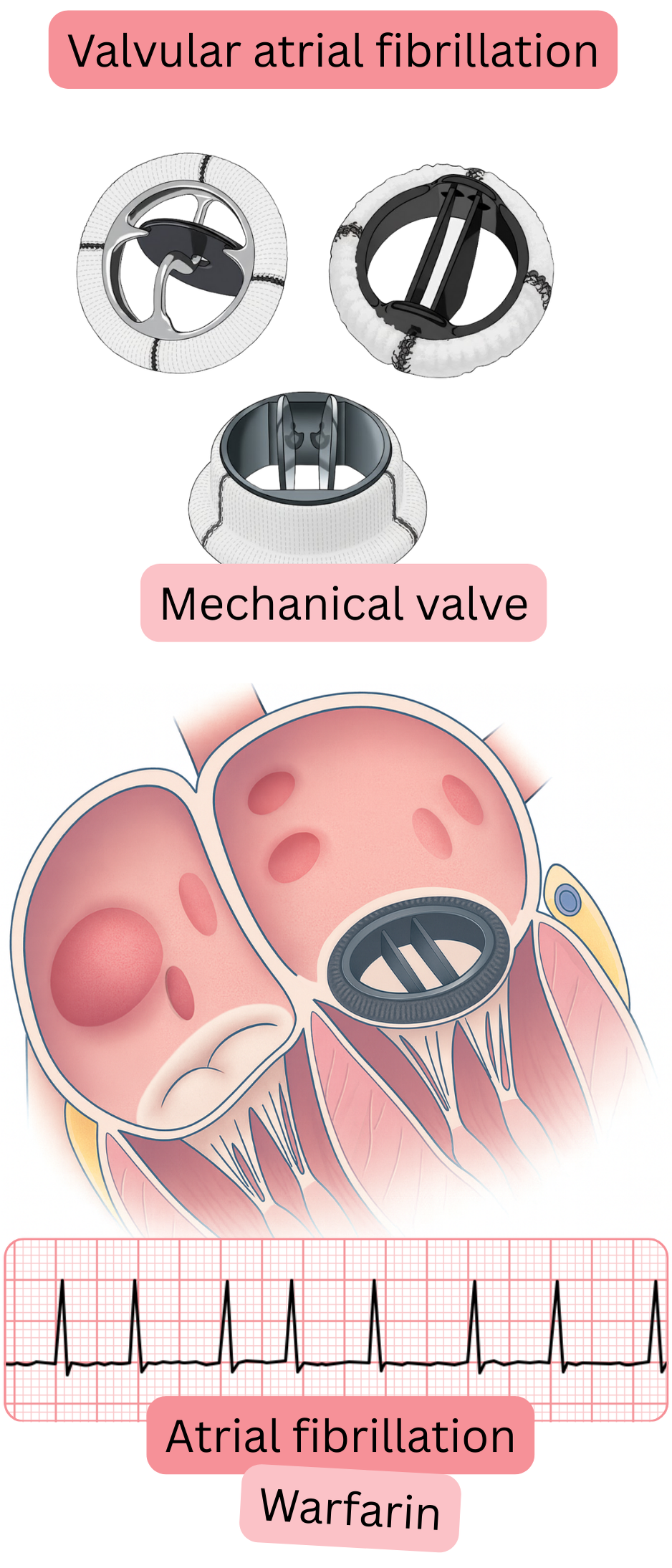
Every mechanical valve is a highly thrombogenic material; therefore, every patient, regardless of the presence of atrial fibrillation (AF), must take anticoagulant therapy—specifically Warfarin (not NOAC).
Warfarin is more effective because it blocks the coagulation cascade at four levels.
Approximately 0.01% of the population has a mechanical valve.
AF occurs in 30–40% of patients with a mechanical valve.
The risk of mechanical valve thrombosis after discontinuation of Warfarin gradually increases up to 20–40% per year.
Prosthetic valves are divided into:
The main advantage of a mechanical valve compared with a bioprosthetic valve is
Mechanical valve:
Bioprosthetic valve:
| Anticoagulant Therapy and Mechanical Valve | Class |
|---|---|
| In patients with atrial fibrillation (AF) and a mechanical valve (valvular AF), Warfarin is always indicated, regardless of the CHA2DS2-VA score. | I |
| In patients with AF after implantation of a bioprosthetic valve, Warfarin is indicated for the first 3 months; thereafter, anticoagulant therapy (NOAC or Warfarin) is indicated according to the CHA2DS2-VA score. | I |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
