
In valvular atrial fibrillation (AF), thrombus formation may occur:
In valvular AF:
In non-valvular AF, thrombus formation may occur:
The trigger for AF is most commonly located:
27 % of patients with recurrent AF after ablation or with AF refractory to medical therapy
If long-term anticoagulation therapy is contraindicated in a patient with AF,
Function of the left atrial appendage:
| Percutaneous Left Atrial Appendage Occlusion (Indications) |
|---|
Spontaneous major bleeding from an irreversible source:
|
Spontaneous major bleeding due to irreversible:
|
| Recurrent major bleeding due to unavoidable falls. |
| Intolerance to anticoagulation therapy |
| Low compliance (patient does not take anticoagulation therapy) |
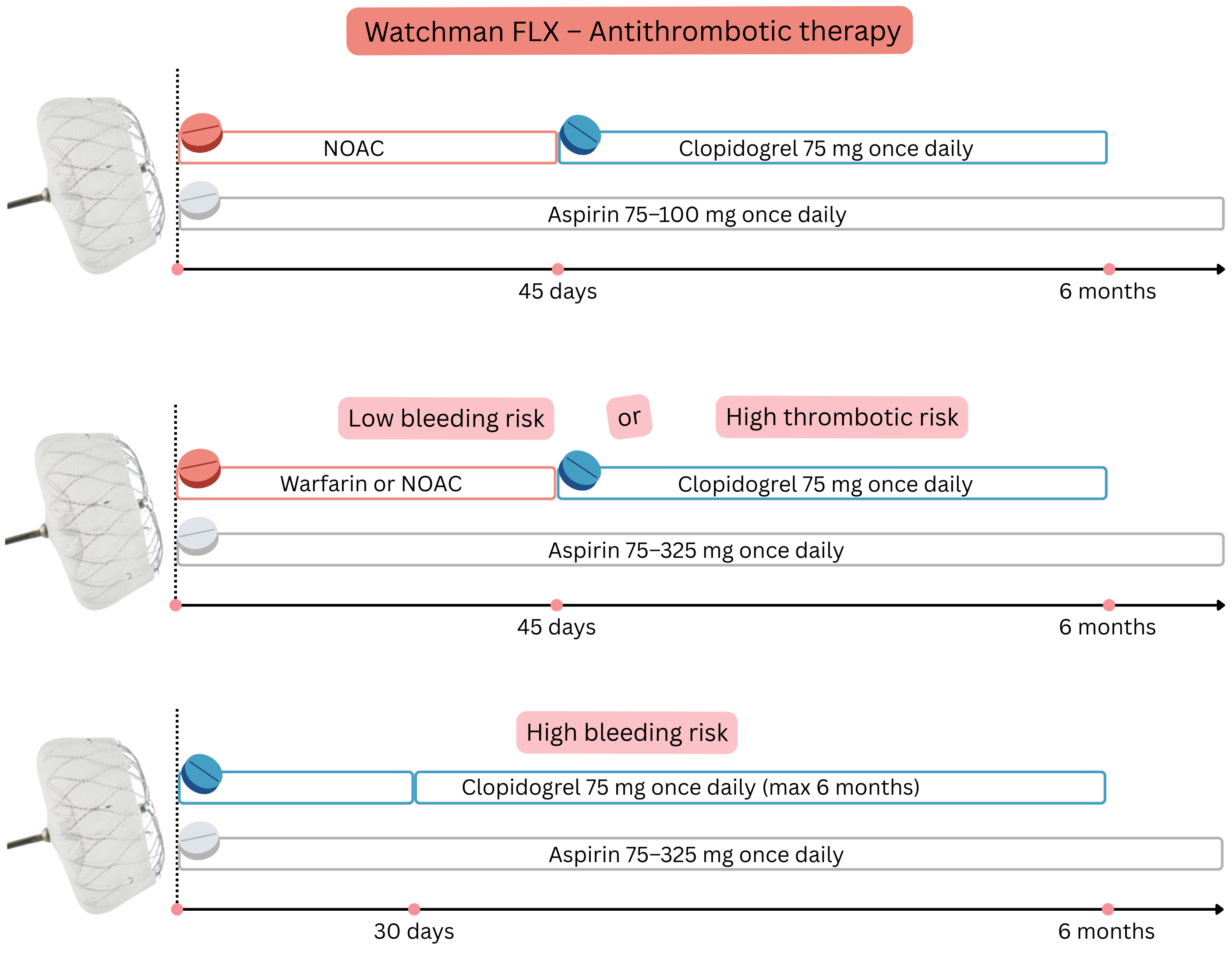
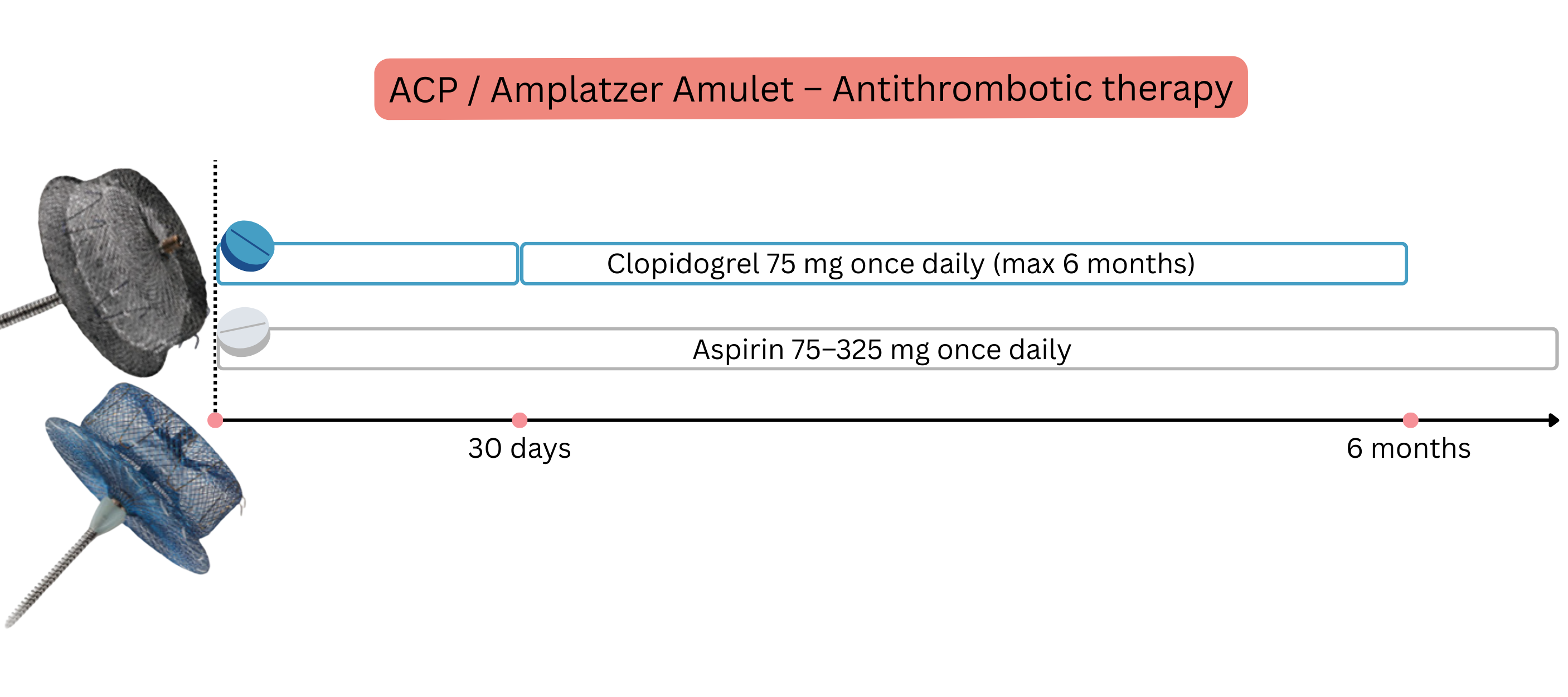
After appendage closure using an occluder (e.g. Watchman), patients must continue for 6 months:
| Percutaneous Left Atrial Appendage Occlusion (Contraindications) |
|---|
| Inability to administer short-term anticoagulation or antiplatelet therapy |
| Thrombus in the atria or ventricles. |
| Valvular atrial fibrillation |
| Allergy to occluder material (nitinol, nickel, titanium) |
Left atrial appendage closure in AF with CHA₂DS₂-VA score ≥ 2
Anticoagulation therapy after surgical closure remains indicated because thrombi may also form outside the appendage.
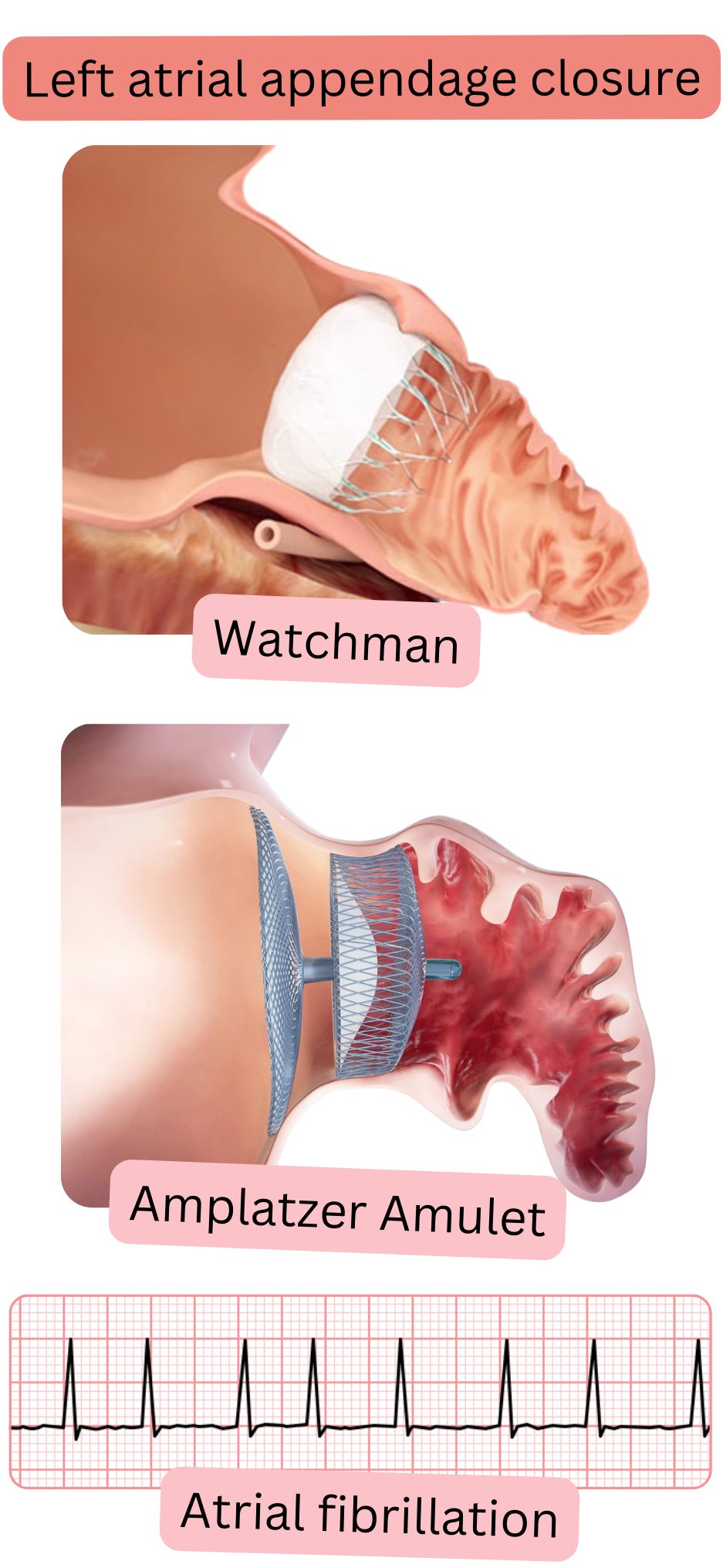
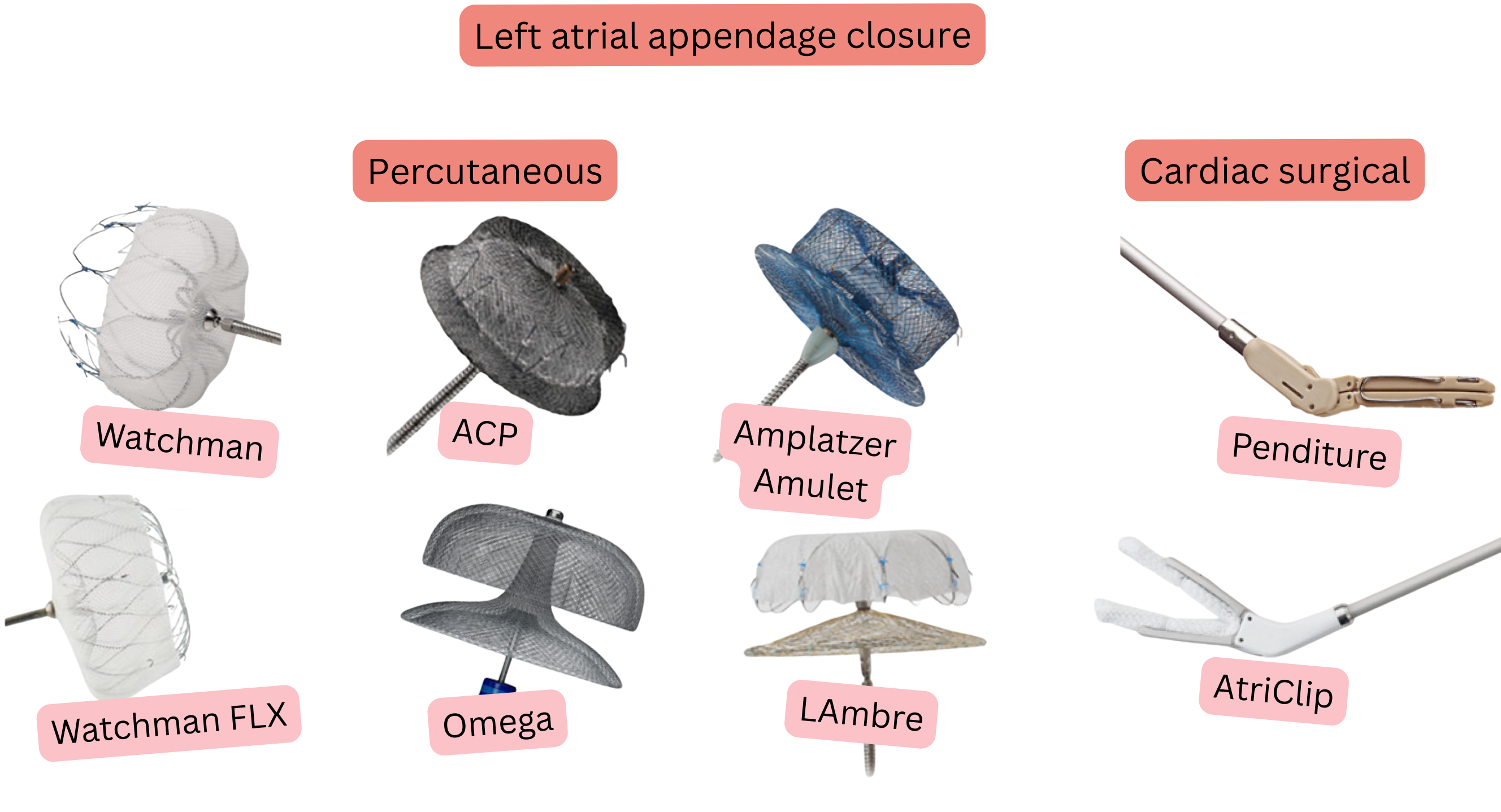
The left atrial appendage can be closed in 3 ways:
Occlusion (percutaneous appendage closure)
Exclusion (surgical appendage closure)
Excision (surgical removal of the appendage)
| Left Atrial Appendage Occlusion | |||
|---|---|---|---|
| Situation | When to close the appendage | Method | Post-procedural therapy |
| Valvular AF (mitral stenosis, mechanical valve) | Only during concomitant cardiac surgery, never as a standalone procedure | Surgical | Warfarin (lifelong) |
| Non-valvular AF with contraindication to anticoagulation therapy | Appendage closure may be considered to reduce embolic risk | Percutaneous occluder (Watchman, Amplatzer) | 6 months dual therapy → then lifelong aspirin |
| Non-valvular AF during cardiac surgery | As an adjunct during planned surgery | Surgical | Anticoagulation therapy according to CHA2DS2-VA |
Percutaneous left atrial appendage occlusion is an invasive procedure associated with a complication rate of approximately 2–4 %.
| Percutaneous Left Atrial Appendage Occlusion | Class |
|---|---|
| In patients with non-valvular AF and CHA2DS2-VA ≥ 2 who have a contraindication to long-term anticoagulation therapy, percutaneous left atrial appendage occlusion may be considered. | IIa |
| In non-valvular AF (low bleeding risk) after percutaneous left atrial appendage occlusion (Watchman FLX), anticoagulation therapy is discontinued after 45 days (if no >5 mm leak is present on transoesophageal echocardiography). | I |
| In non-valvular AF after percutaneous left atrial appendage occlusion, long-term aspirin therapy is recommended. | I |
| Surgical Left Atrial Appendage Closure | Class |
|---|---|
| Surgical left atrial appendage closure is recommended (as adjunctive “anticoagulation” therapy) in all patients with AF undergoing cardiac surgery. | I |
| Thoracoscopic surgical left atrial appendage closure may be considered in patients with a contraindication to long-term anticoagulation therapy who are unsuitable for percutaneous appendage closure. | IIb |
| In non-valvular AF after surgical left atrial appendage closure, anticoagulation therapy is indicated according to the CHA2DS2-VA score. | I |
| In valvular AF after surgical left atrial appendage closure, warfarin is administered regardless of the CHA2DS2-VA score. | I |
In patients after left atrial appendage occlusion or after percutaneous coronary intervention (PCI)
| ARC-HBR Score (Bleeding Risk) |
|---|
Major criteria (1 is sufficient)
|
Minor criteria (≥2 required)
|
ARC-HBR - Academic Research Consortium – High Bleeding Risk. PCI - Percutaneous Coronary Intervention. NOAC – Non-vitamin K Oral Anticoagulant (Dabigatran, Rivaroxaban, Apixaban, Edoxaban). eGFR = estimated Glomerular Filtration Rate. NSAIDs - non-steroidal anti-inflammatory drugs
Low bleeding risk in patients after left atrial appendage occlusion is assessed according to the following table.
| Low Bleeding Risk (after left atrial appendage occlusion) |
|---|
| All criteria must be fulfilled |
| HAS-BLED < 3 |
| ARC-HBR: no major criterion and ≤ 1 minor criterion |
| No previous life-threatening bleeding |
| Stable anticoagulation therapy in the past without complications |
| Normal renal function (CrCl > 50 ml/min) |
| Normal liver function |
| No active gastrointestinal ulceration |
| No recent surgery or traumatic events |
| No anaemia or thrombocytopenia |
| No need for dual antiplatelet therapy (DAPT) for another indication |
DAPT - Dual Antiplatelet Therapy (Aspirin + Clopidogrel). CrCl – creatinine clearance
High thrombotic risk in patients after left atrial appendage occlusion is assessed according to the following table.
| High Thrombotic Risk (after left atrial appendage occlusion) |
|---|
| One parameter is sufficient |
| CHA₂DS₂-VA ≥ 5 |
| Previous appendage thrombus |
| Thrombophilias (factor V Leiden, protein C/S deficiency, antiphospholipid syndrome) |
| Left atrial dilatation (>50 mm, LAVI >40 ml/m²) |
| Persistent atrial fibrillation |
| Left ventricular ejection fraction (<40 %) |
| Spontaneous echocontrast in the left atrium |
| History of embolization during anticoagulation therapy |
| Obesity + diabetes + hypertension + age >75 years (synergistic effect) |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
