
Atrial fibrillation (AF) develops in structurally and electrically altered atria.
| Main Mechanisms of Atrial Fibrillation in Inherited Arrhythmic Syndromes and Cardiomyopathies | ||
|---|---|---|
| Diagnoses | Atrial Changes | Mechanism of AF Development |
| HCM DCM ARVC |
Structural atrial changes (dilatation, fibrosis, increased wall stress) |
Structural remodelling creates an arrhythmogenic substrate for atrial arrhythmias and atrial fibrillation. |
|
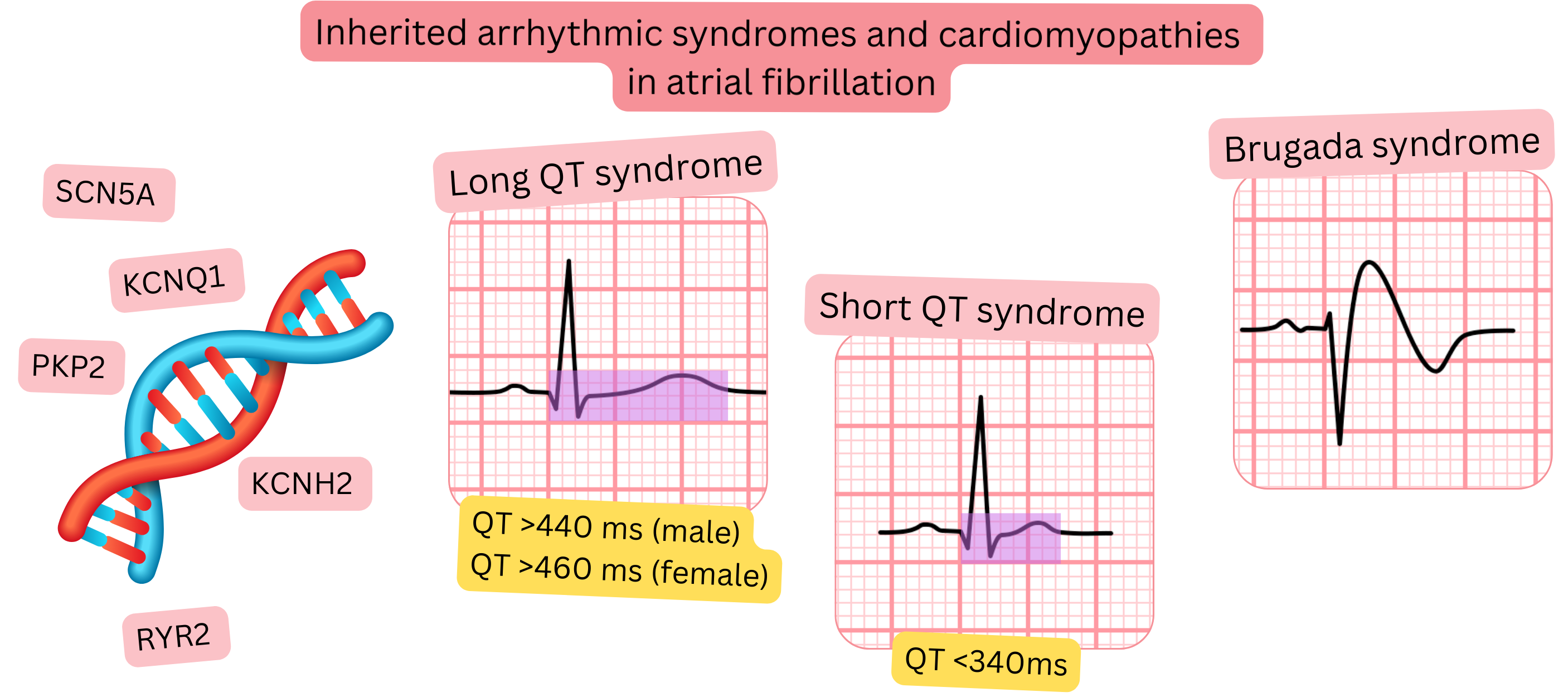
Long QT syndrome Short QT syndrome Brugada syndrome CPVT WPW syndrome |
Electrical and ionic alterations in the atria | Ion channel dysfunction and impaired electrical stability increase atrial vulnerability to arrhythmias and AF. |
|
Gene mutations (SCN5A, KCNQ1, KCNH2, RYR2, etc.) |
Genetic alterations affecting the atrial myocardium | Mutations involve not only the ventricles but also the atria, thereby creating an arrhythmogenic substrate for AF. |
| HCM DCM |
Chronic overload and diastolic dysfunction | Elevated filling pressures lead to left atrial dilatation and formation of a stable substrate for AF. |
| CPVT Long QT syndrome |
Autonomic dysregulation | Adrenergic stress and impaired autonomic regulation promote atrial arrhythmias and AF. |
ARVC – Arrhythmogenic right ventricular cardiomyopathy, CPVT – Catecholaminergic polymorphic ventricular tachycardia, DCM – Dilated cardiomyopathy, AF – Atrial fibrillation, HCM – Hypertrophic cardiomyopathy
Arrhythmic syndromes and cardiomyopathies may also arise due to gene mutations.
| Genetic Mutations and Their Association with Atrial Fibrillation | |||
|---|---|---|---|
| Gene Mutation | AF Prevalence | Associated Cardiac Diagnoses | Mechanism of AF |
| SCN5A | 20–40 % |
Brugada syndrome DCM (electrical phenotype) Genetic AF |
Electrical atrial instability. |
| KCNQ1 | 10–30 % |
Long QT syndrome type 1 Familial AF |
Atrial repolarization abnormality. |
| KCNH2 (HERG) | 10–25 % | Long QT syndrome type 2 | Increased atrial vulnerability. |
| RYR2 | 5–15 % | CPVT | Adrenergic Ca2+ discharges → ectopy. |
| CACNA1C | 30–50 % |
Brugada phenotype Timothy syndrome Atrial arrhythmias |
Ca2+ channel dysfunction → atrial excitability. |
| MYH7 | 20–35 % |
HCM DCM LVNC |
Atrial fibrosis and dilatation. |
| MYBPC3 | 20–35 % | HCM | Atrial fibrosis in HCM. |
| LMNA | 45–70 % | Laminopathy (DCM + AV block) | Atrial remodelling. |
| TNNI3 | 15–30 % | HCM | Atrial remodelling in hypertrophy. |
| TNNT2 | 20–35 % |
HCM DCM |
Atrial fibrosis. |
| PLN | 15–25 % |
DCM ARVC-like phenotype |
Electrical atrial instability. |
| DSP | 10–25 % | ARVC | Atrial fibrotic remodelling. |
| PKP2 | 10–20 % | ARVC | Atrial arrhythmias during disease progression. |
| PRKAG2 | 20–40 % |
Glycogen storage cardiomyopathy Hypertrophy + WPW phenotype |
Atrial hypertrophy and pre-excitation. |
| GLA | 30–60 % | Fabry disease | Atrial fibrosis. |
ARVC – Arrhythmogenic right ventricular cardiomyopathy, CPVT – Catecholaminergic polymorphic ventricular tachycardia, DCM – Dilated cardiomyopathy, AF – Atrial fibrillation, HCM – Hypertrophic cardiomyopathy, LVNC – Left ventricular non-compaction cardiomyopathy, WPW – Wolff–Parkinson–White syndrome
In the following table, you can review the prevalence of AF in arrhythmic syndromes and cardiomyopathies.
| Genetic and Inherited Arrhythmological Syndromes – Prevalence, AF Risk, Contraindications, and Anticoagulation | ||||
|---|---|---|---|---|
| Diagnosis | Prevalence | AF Prevalence | Contraindications | Anticoagulation |
| Long QT syndrome | 1 : 2 000 | 2–29 % | QT-prolonging drugs (1) | According to CHA2DS2-VA |
| Short QT syndrome | 1 : 100 000 | 18–70 % | – | According to CHA2DS2-VA |
| Brugada syndrome | 1 : 5 000 | 6–53 % | Class IC anti-arrhythmic drugs | According to CHA2DS2-VA |
| CPVT | 1 : 50 000 | 11–37 % | – | According to CHA2DS2-VA |
| HCM | 1 : 500 | 17–30 % | Class IC anti-arrhythmic drugs | Always (NOAC or warfarin) |
| ARVC | 1 : 2 000 | 9–30 % | – | According to CHA2DS2-VA |
| DCM (LMNA mutation) | 1 : 400 | 25–49 % | – | According to CHA2DS2-VA |
| WPW syndrome | 1 : 500 | 7–50 % | AV node–blocking drugs (2) | According to CHA2DS2-VA |
CPVT – Catecholaminergic polymorphic ventricular tachycardia, HCM – Hypertrophic cardiomyopathy, ARVC – Arrhythmogenic right ventricular cardiomyopathy, DCM – Dilated cardiomyopathy.
1 In Long QT syndrome, QT-prolonging drugs are contraindicated:
- IA: Quinidine, Procainamide, Disopyramide
- III: Amiodarone, Sotalol, Dofetilide, Ibutilide, Dronedarone
- IC: Propafenone, Flecainide (relative contraindication)
2 AV node–blocking drugs: Beta-blockers, Digoxin, Verapamil, Diltiazem, Amiodarone, Adenosine
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
