Endocrinopathies and Atrial Fibrillation
Endocrine disorders lead to hormonal and metabolic changes, which also result in atrial remodelling, thereby progressively creating a substrate for atrial fibrillation (AF).
Adequate treatment of the endocrine disorder is essential for the prevention and management of AF.
In every newly diagnosed AF, thyroid function (TSH, fT4) must be assessed.
Amiodarone induces thyroid dysfunction in 15–20% of patients after 1–3 months of therapy:
- it more frequently causes hypothyroidism than hyperthyroidism in a 4:1 ratio.
An amiodarone 300 mg bolus may transiently alter fT4 or TSH levels,
- hormone levels return to baseline within 48 hours.
- it does not cause clinically relevant hypothyroidism or hyperthyroidism (in patients without pre-existing thyroid disease).
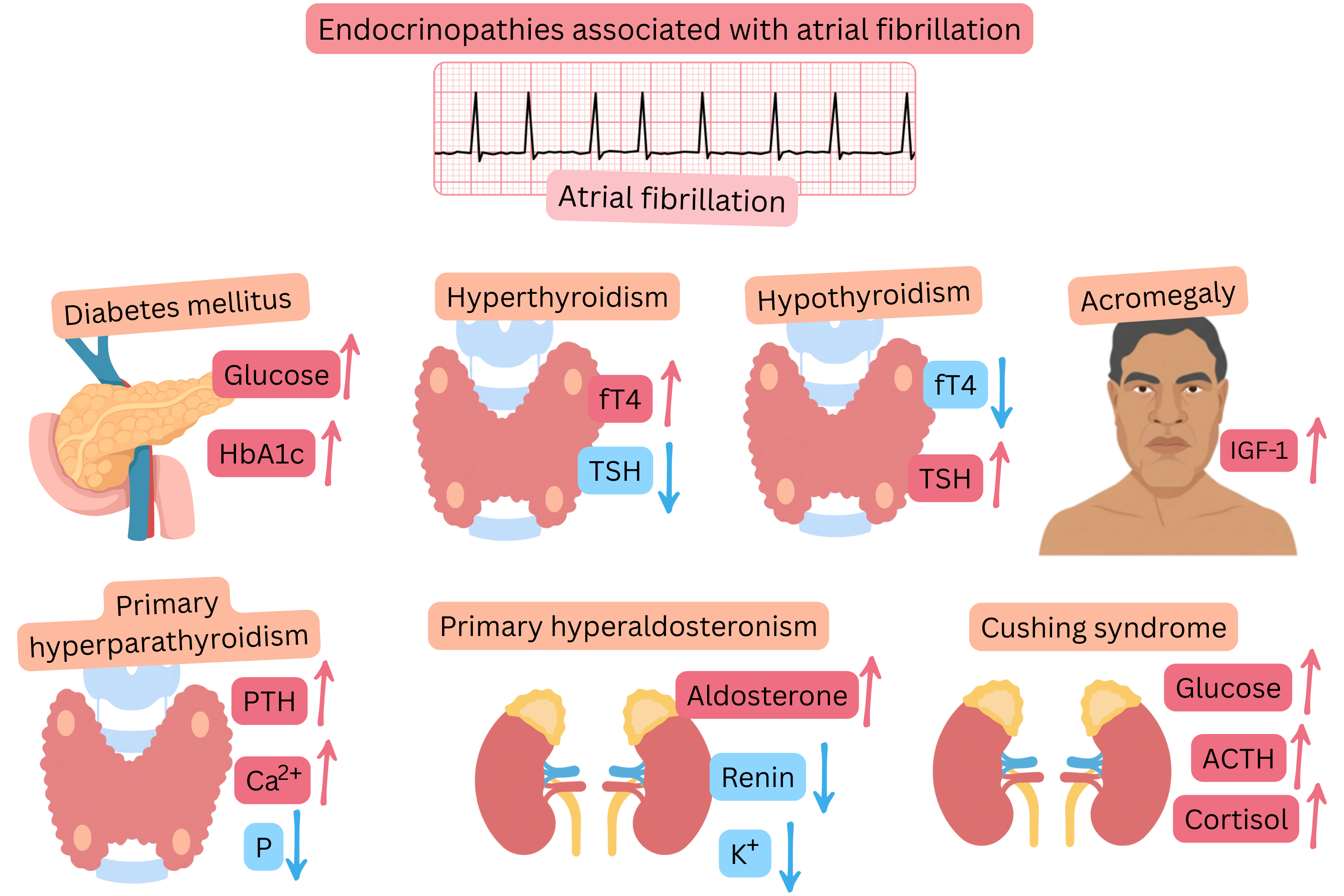
Endocrine disorders associated with AF:
| Endocrine disorders associated with atrial fibrillation |
Hypothyroidism
- Prevalence: 1%
- Diagnosis: fT4, TSH
- AF prevalence: 1%
- AF mechanism: Diastolic dysfunction → atrial dilatation and remodelling
|
Hyperthyroidism
- Prevalence: 1%
- Diagnosis: fT4, TSH
- AF prevalence: 10–25%
- AF mechanism: T4/T3 increase beta-adrenergic receptor sensitivity → atrial remodelling
|
Acromegaly
- Prevalence: 1/10 000
- Diagnosis: Growth hormone (GH)
- AF prevalence: 7%
- AF mechanism: Atrial enlargement and fibrosis
|
| Endocrine disorders associated with atrial fibrillation |
Primary hyperaldosteronism
- Prevalence: 5–10% in hypertensive patients, 20–30% in resistant hypertension
- Diagnosis: Hypokalaemia, poorly controlled hypertension, renin
- AF prevalence: 5–15%, in resistant hypertension 15–25%
- AF mechanism: Hypertension and hypokalaemia → atrial dilatation and electrical remodelling
|
Diabetes mellitus (DM)
- Prevalence: 10% (DM2 = 90%, DM1 = 10%)
- Diagnosis: Fasting glucose, HbA1c
- AF prevalence: 5–15%
- AF mechanism: Hyperglycaemia → diastolic dysfunction → atrial dilatation and remodelling
|
Primary hyperparathyroidism
- Prevalence: 0.1%
- Diagnosis: Hypercalcaemia, hypophosphataemia, ↑ parathyroid hormone
- AF prevalence: 5–15%
- AF mechanism: Hypercalcaemia → electrical remodelling → ectopic activity + atrial remodelling
|
Cushing syndrome
- Prevalence: 1/100 000 (80% central, 20% peripheral)
- Diagnosis: ACTH, 24-hour urinary cortisol, dexamethasone test
- AF prevalence: 5–10%
- AF mechanism: Cortisol overproduction → hypertension, LV hypertrophy, atrial remodelling
|
| Endocrinopathies and atrial fibrillation |
Class |
In every patient with newly diagnosed atrial fibrillation, the following are recommended:
- TSH, fT4 (thyroid parameters)
- Fasting glucose, HbA1c (diabetes mellitus)
- K (primary hyperaldosteronism)
- Ca, P (primary hyperparathyroidism)
|
I |