ECG and Atrial Fibrillation
Atrial fibrillation (AF) begins as paroxysmal AF episodes (spontaneously terminating within 7 days) that are triggered by an atrial arrhythmia:
- Atrial premature beats, or
- Rapid atrial activity, which is further divided into:
- Atrial premature beats in runs (3–5 beats)
- Non-sustained atrial tachycardia (<30 s)
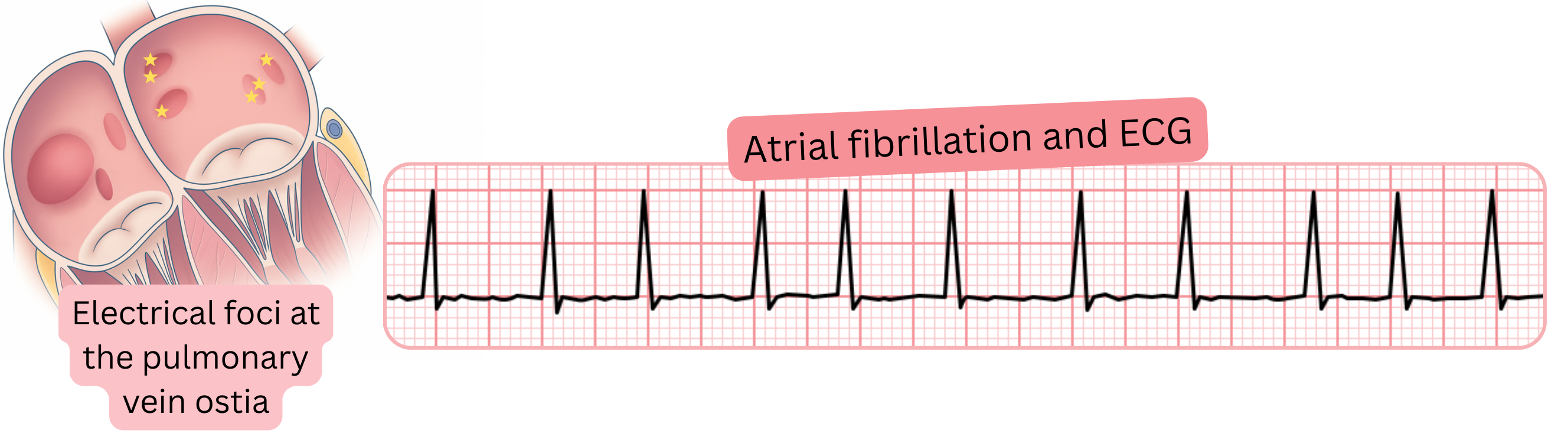
The atrial arrhythmia that triggers paroxysmal AF originates from the region of the pulmonary vein ostia. These atrial arrhythmias can sometimes be captured on a 12-lead ECG.
Atrial premature beats originating from the pulmonary vein ostia can sometimes be identified by the P wave on a 12-lead ECG. These premature beats do not necessarily have to be followed by an AF paroxysm.
Rapid atrial activity originating from the pulmonary vein ostia has a rate of 200–220/min and is often followed by an AF paroxysm. During rapid atrial activity, P waves are almost always concealed within the preceding T wave and are therefore difficult to evaluate on a 12-lead ECG. Rapid atrial activity refers to the above-mentioned
- atrial premature beats in runs (3–5 beats) or
- non-sustained atrial tachycardia (<30 s).
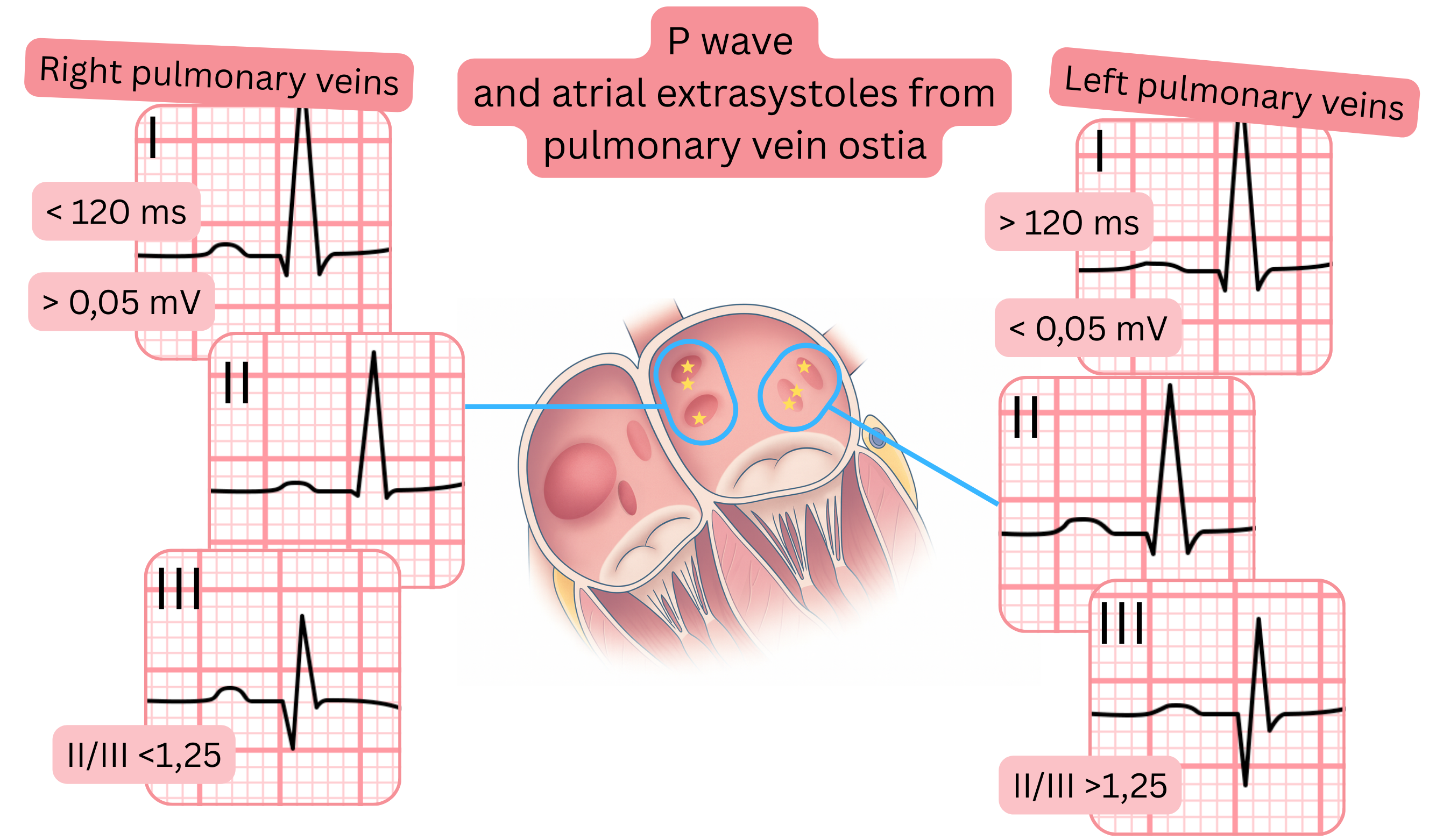
| ECG and atrial premature beats from the pulmonary veins |
| ECG features |
Left-sided pulmonary veins |
Right-sided pulmonary veins |
| P-wave width |
>120 ms |
<120 ms |
| Amplitude |
II/III >1.25 |
II/III <1.25 |
| Amplitude |
I <0.05 mV (mm) |
I >0.05 mV (mm) |
ECG during an AF episode
- On the ECG, P waves are absent, and fibrillatory waves are present. During an AF episode, the atria fibrillate at an irregular rate of 300–600/min. The SA node is suppressed because it is driven by a higher impulse frequency than it can generate—overdrive suppression occurs:
- an electrophysiological phenomenon in which the automaticity of pacemaker cells is suppressed because the pacemaker cells are stimulated at a faster rate than their intrinsic spontaneous rate.
- QRS complexes are irregular because the AV node acts as a filter. Irregular atrial impulses at 300–600/min are conducted through the AV node to the ventricles at a lower, irregular rate, most commonly <100/min. The AV node has:
- A long effective refractory period (ERP) that prolongs at higher stimulation rates (so-called use-dependent or rate-dependent conduction slowing).
- Decremental conduction—the higher the frequency of incoming impulses, the slower their conduction through the AV node.
- Rarely (<1 %), the RR interval during an AF episode may be regular.
- This phenomenon may occur if the patient has third-degree AV block with AF and a concomitant junctional or ventricular escape rhythm.
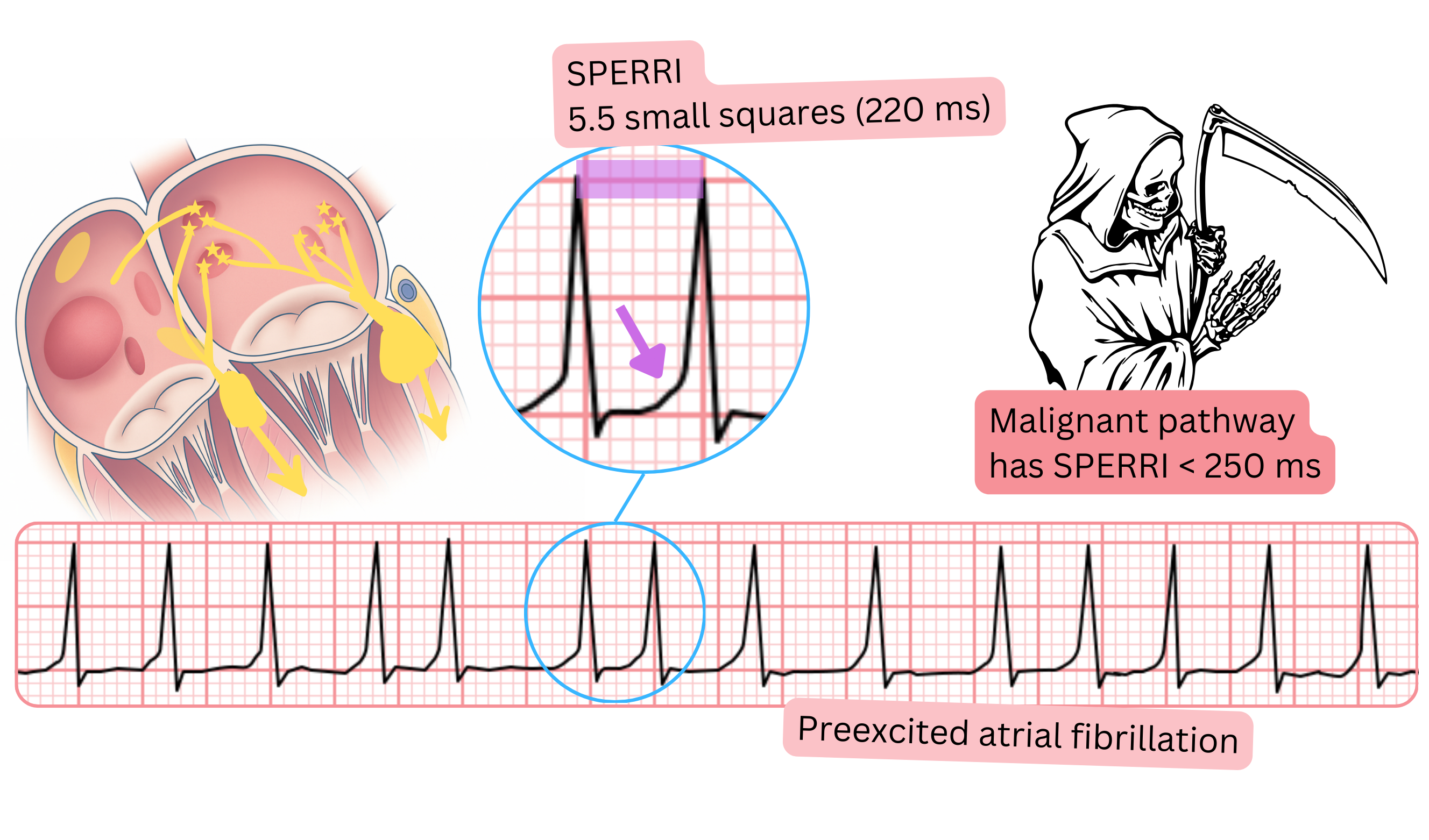
ECG and pre-excited AF
- Pre-excited AF is AF with a delta wave on ECG. The delta wave indicates that the patient has an anterograde accessory pathway.
- An accessory pathway is present in <1 % of the population.
- If atrial impulses at 300–600/min were conducted to the ventricles, the patient would develop ventricular fibrillation, which is a life-threatening condition.
- This may occur if the patient has AF and a malignant anterograde accessory pathway. The risk of ventricular fibrillation increases if the patient receives drugs that slow conduction through the AV node.
- A malignant accessory pathway is defined by the SPERRI parameter (<250 ms).
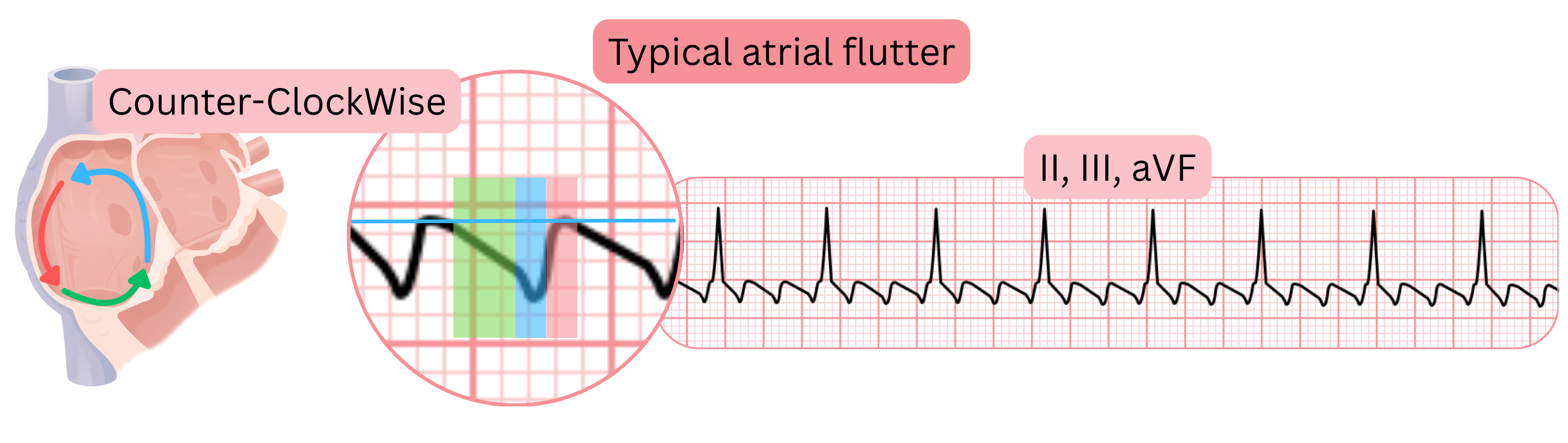
ECG and atrial flutter
- 20 % of patients with AF also have atrial flutter (typical or atypical).
- Therefore, one ECG may show AF and another ECG may show atrial flutter in the same patient.
- Typical atrial flutter produces characteristic flutter waves in the inferior leads (II, III, aVF), V1, and V6, because the impulse circulates in a re-entry circuit around the right atrium through the cavotricuspid isthmus.
- Atypical atrial flutter produces flutter waves that differ from typical flutter because the impulse circulates in a different re-entry circuit. In AF patients, atypical flutter most commonly arises in the left atrium.
| ECG and atrial fibrillation |
| The AF trigger—an atrial arrhythmia (atrial premature beats or rapid atrial activity) originating from the pulmonary vein ostia—can sometimes be captured and localized using a 12-lead ECG. |
| An AF episode produces irregular fibrillatory waves at 300–600/min and irregular RR intervals on ECG. P waves are absent. |
| An AF episode may have regular RR intervals if third-degree AV block and a junctional or ventricular escape rhythm are present; this is rare (<1 %). |
| Pre-excited AF produces a delta wave on ECG during an AF episode. If the accessory pathway is malignant, the patient may develop ventricular fibrillation. A malignant accessory pathway has SPERRI <250 ms. |
| Atrial flutter produces flutter waves on ECG. 20 % of patients with AF also have atrial flutter; therefore, these arrhythmias may alternate in the same patient. |

