CHA₂DS₂-VA Score and Stroke Risk in Atrial Fibrillation
The largest amount of clinical data is available for the CHA2DS2-VASc score.
- in which female sex is one of the parameters as a risk factor.
- However, female sex is a risk factor at older age > 65 years (mainly due to hormonal changes).
- and the question remains which sex should be used in a patient after transgender hormonal and surgical transition to the opposite sex.
- Therefore, in 2024 the CHA2DS2-VA score started to be used,
- which removed female sex as a risk factor.
The risk of thromboembolism (TE) and stroke is almost identical,
- regardless of whether it is calculated using the CHA2DS2-VASc or the CHA2DS2-VA score.
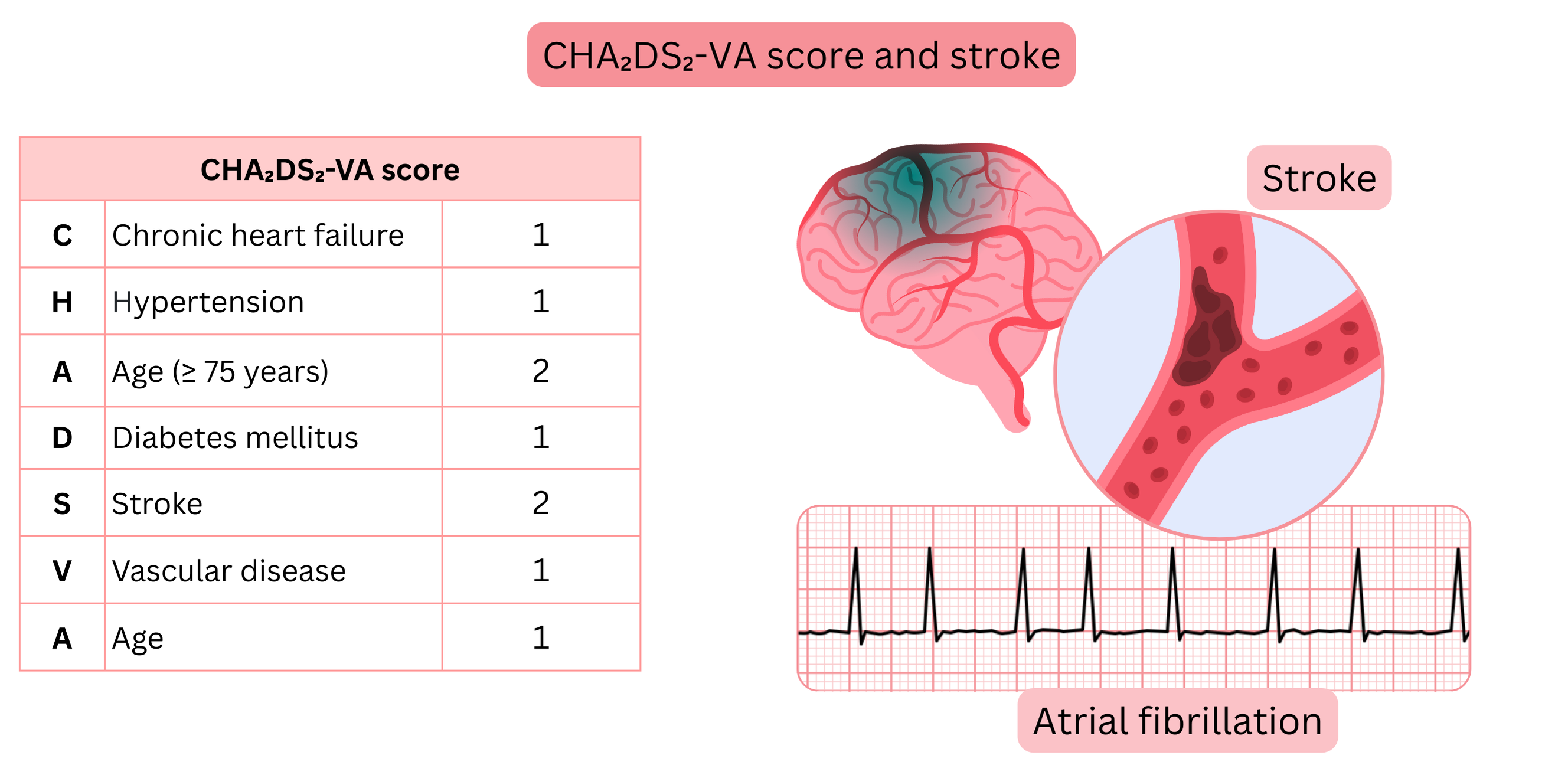
| CHA2DS2-VA score |
| Parameter |
Criteria (at least 1 criterion must be met) |
Points |
Chronic heart failure
(Chronic heart failure) |
- Symptoms or parameters of heart failure
- regardless of ejection fraction (HFrEF, HFmrEF, HFpEF).
|
1 |
Hypertension
(Arterial hypertension) |
- Use of antihypertensive medication
- Blood pressure > 140/90 mmHg
- (at least 3 home measurements at intervals ≥ 1 day)
|
1 |
Age (≥ 75 years)
(Age ≥ 75 years) |
|
2 |
Diabetes mellitus
(Diabetes mellitus) |
- Type 1 or type 2 diabetes mellitus
- Fasting plasma glucose > 7 mmol/l
- HbA1c > 6,5 %
- Random plasma glucose > 11 mmol/l
|
1 |
Stroke
(Stroke) |
- Ischemic stroke
- Transient ischemic attack
- Thromboembolism
|
2 |
Vascular disease
(Vascular disease) |
- Coronary artery disease
- Angina pectoris
- Post-myocardial infarction
- Post-coronary revascularization
- CT coronary angiography (> 50 % stenosis)
- Positive exercise stress test
- Peripheral arterial disease
- Intermittent claudication
- Post-revascularization
- Aortic vascular disease
- Post-aortic intervention
- Atherosclerotic plaque in the aorta (≥ 4 mm)
|
1 |
Age (65–74 years)
(Age 65–74 years) |
|
1 |
Ischemic stroke (IS)
- Is the main statistical parameter used in the development of thromboembolic risk scoring systems in atrial fibrillation (AF).
- Ischemic stroke causes symptoms in the patient that are diagnosed by the healthcare system and can be linked to AF.
- Other thromboembolic events, for example:
- hematuria, lower limb ischemia, or angina pectoris, are more difficult for the healthcare system to associate with AF.
- Therefore, the term thromboembolic risk in AF generally refers to the risk of embolic ischemic stroke.
|
Atrial Fibrillation and Stroke Risk According to the CHA2DS2-VA Score (1 year)
|
| CHA2DS2-VA Score |
Stroke Risk (without NOAC) |
Stroke Risk (with NOAC) |
| 0 | 0,5 % | 0,2 % |
|---|
| 1 | 1,5 % | 0,5 % |
|---|
| 2 | 3 % | 1,0 % |
|---|
| 3 | 5 % | 1,8 % |
|---|
| 4 | 7 % | 2,6 % |
|---|
| 5 | 11 % | 3,9 % |
|---|
| 6 | 14 % | 5,4 % |
|---|
| 7 | 15 % | 5,1 % |
|---|
| 8 | 19 % | 6,8 % |
|---|
There is a consensus that anticoagulant therapy (OAC) in AF is indicated,
- if the risk of thromboembolism (ischemic stroke) is > 1–2 % per year.
In anticoagulant therapy (OAC) and AF, the following exceptions apply:
- OAC (preferably NOAC, or Warfarin) is always indicated regardless of the CHA2DS2-VA score if the patient has:
- Hypertrophic cardiomyopathy
- Cardiac amyloidosis
- OAC (always Warfarin) is always indicated regardless of the CHA2DS2-VA score if the patient has:
- Mitral stenosis (moderate or severe)
- A mechanical valve.
| Thromboembolism (Ischemic Stroke) and Atrial Fibrillation |
Class |
Oral anticoagulant therapy in patients with AF is indicated according to the CHA2DS2-VA score,
- regardless of whether AF is paroxysmal, persistent, permanent, symptomatic, or asymptomatic.
|
I |
| Oral anticoagulant therapy is recommended in patients with AF and CHA2DS2-VA score ≥ 2. |
I |
| Oral anticoagulant therapy should be considered in patients with AF and CHA2DS2-VA score = 1. |
IIa |
Oral anticoagulant therapy (preferably NOAC) is indicated in all patients regardless of the CHA2DS2-VA score with
- hypertrophic cardiomyopathy or
- cardiac amyloidosis
|
I |
Warfarin as anticoagulant therapy is indicated in all patients regardless of the CHA2DS2-VA score with
- a mechanical valve or
- mitral stenosis (moderate or severe)
|
I |
| Oral anticoagulant therapy may be considered in patients with subclinical AF (with detected AHRE). |
IIb |
| It is recommended to reassess the CHA2DS2-VA score regularly (every 6–12 months), or when the patient’s condition changes (reaches 65 years of age, develops hypertension, diabetes mellitus, etc.). |
I |
AHRE (Atrial High Rate Episodes)
- are diagnosed using CIED (Cardiac Implantable Electronic Devices),
- which have an atrial lead that senses the electrical activity of the atria.
- AHRE is an episode of atrial tachyarrhythmia lasting > 5 min and with a rate > 170/min.
- AHRE detected by a CIED atrial lead may represent:
- atrial flutter, atrial tachycardia, atrial fibrillation.

