
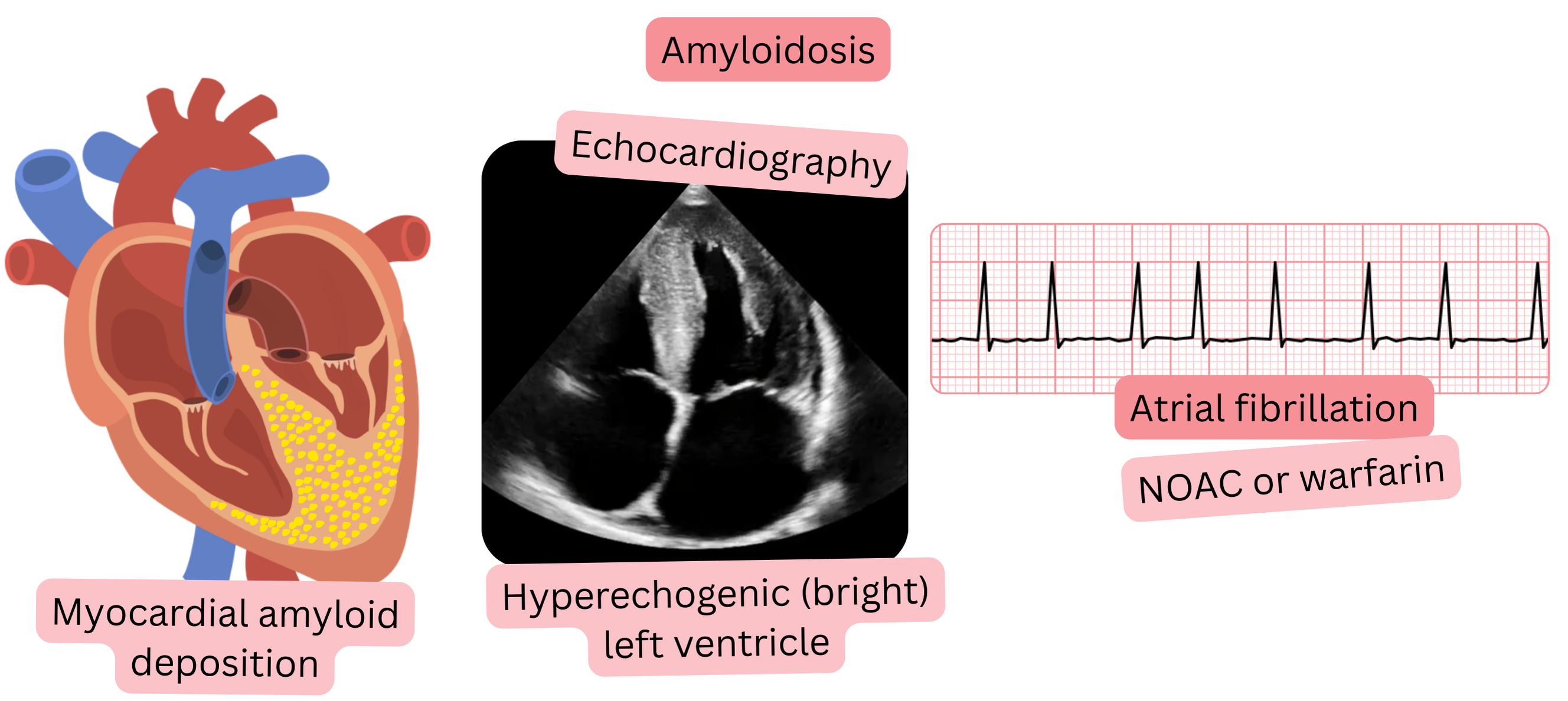
Amyloidosis is a systemic infiltrative disease in which amyloid is deposited in the extracellular space of the myocardium; this condition is referred to as cardiac amyloidosis.
Cardiac amyloidosis
Amyloidosis may be
Aortic stenosis is present in 10–20% of patients with cardiac amyloidosis.
AF is present in 50–70% of patients with cardiac amyloidosis.
Cardiac amyloidosis with AF carries a thromboembolic risk of 5–10% per year
| Anticoagulant Therapy and Cardiac Amyloidosis | Class |
|---|---|
| In patients with cardiac amyloidosis and atrial fibrillation, anticoagulant therapy (preferably NOAC) is always indicated, regardless of the CHA2DS2-VA score. | I |
Cardiac amyloidosis produces characteristic findings on ECG and transthoracic echocardiography, which are summarized in the table below.
The following modalities are used for definitive diagnosis of cardiac amyloidosis:
| Cardiac Amyloidosis – ECG and Transthoracic Echocardiography (TTE) | |
|---|---|
| Investigation | Characteristic findings |
| ECG |
|
| TTE |
|
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
