
Anticoagulation therapy in atrial fibrillation (AF) is divided into 2 main groups:
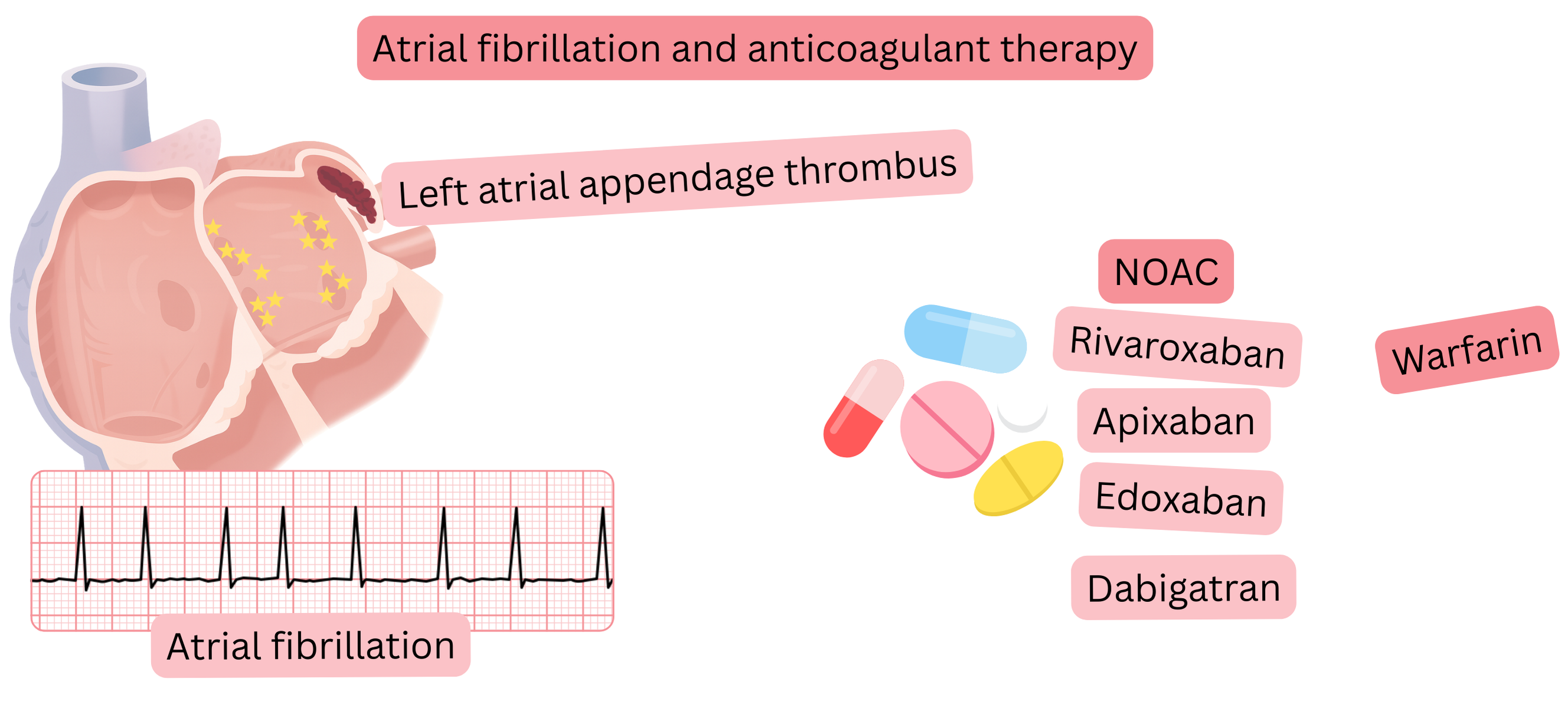
Vitamin K antagonists inhibit coagulation factors (II, VII, IX, X) and include:
Warfarin is the most commonly used vitamin K antagonist.
The main disadvantage of warfarin is the need for regular INR monitoring, which should be maintained between 2–3,
In clinical practice, NOAC are used more frequently, as INR monitoring is not required. In clinical trials they demonstrate:
There are 4 NOAC available; three inhibit coagulation factor Xa and one inhibits factor IIa:
In patients with body weight >120 kg or BMI >40 kg/m2
| NOAC (Non-Vitamin K Oral Anticoagulants) | |||
|---|---|---|---|
| NOAC | Standard dosing |
Dose reduction criteria | Reduced dose |
| Apixaban (Eliquis) |
5 mg twice daily |
Dose reduction is recommended if at least two of the following are present:
|
2.5 mg twice daily |
| Dabigatran (Pradaxa) |
150 mg twice daily |
Dose reduction is recommended if at least one of the following is present:
|
110 mg twice daily |
| Edoxaban (Lixiana, Savaysa) |
60 mg once daily |
Dose reduction is recommended if at least one of the following is present:
|
30 mg once daily |
| Rivaroxaban (Xarelto) |
20 mg once daily |
Dose reduction is recommended if:
|
15 mg once daily |
CrCl – creatinine clearance, GERD – gastro-oesophageal reflux disease
| Adverse effects of NOAC | |
|---|---|
| Adverse effect | Annual risk (%) |
| Minor bleeding (epistaxis, bruising) | 10 – 15 % |
| Dyspepsia (especially with dabigatran) | 5 – 10 % |
| Haematuria | 1 – 3 % |
| Anaemia (due to bleeding) | 1 – 3 % |
| Nausea | 1 – 3 % |
| Major bleeding | 1 – 2 % |
| Gastrointestinal bleeding | 1 – 2 % |
| Intracranial bleeding | < 1 % |
| Elevated liver enzymes | < 1 % |
| Allergic / hypersensitivity reactions | < 1 % |
| Renal dysfunction (rarely in dehydration / bleeding) | < 1 % |
| Thrombocytopenia | < 1 % |
Based on clinical trial data, there are 3 clinical situations in which patients with AF should receive anticoagulation irrespective of CHA2DS2-VA score:
The main reason why warfarin is more effective in valvular AF is:
| Anticoagulation therapy and atrial fibrillation | Class |
|---|---|
In valvular atrial fibrillation:
|
I |
| During warfarin therapy, a target INR of 2–3 is recommended. | I |
| Switching from warfarin to NOAC is recommended if anticoagulation is inadequate (Time in Therapeutic Range < 70 %). | I |
| Dose reduction of NOAC is recommended only if dose reduction criteria are fulfilled. | I |
| In patients with body weight >120 kg or BMI >40 kg/m2, warfarin is recommended according to CHA2DS2-VA score. | I |
| In patients with body weight >120 kg or BMI >40 kg/m2, NOAC may be considered according to CHA2DS2-VA score. | IIb |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
