Ablation of Atrial Fibrillation – Principle and Methods
Ablation means removal or deactivation of tissue using heat, cold, or another source of energy.
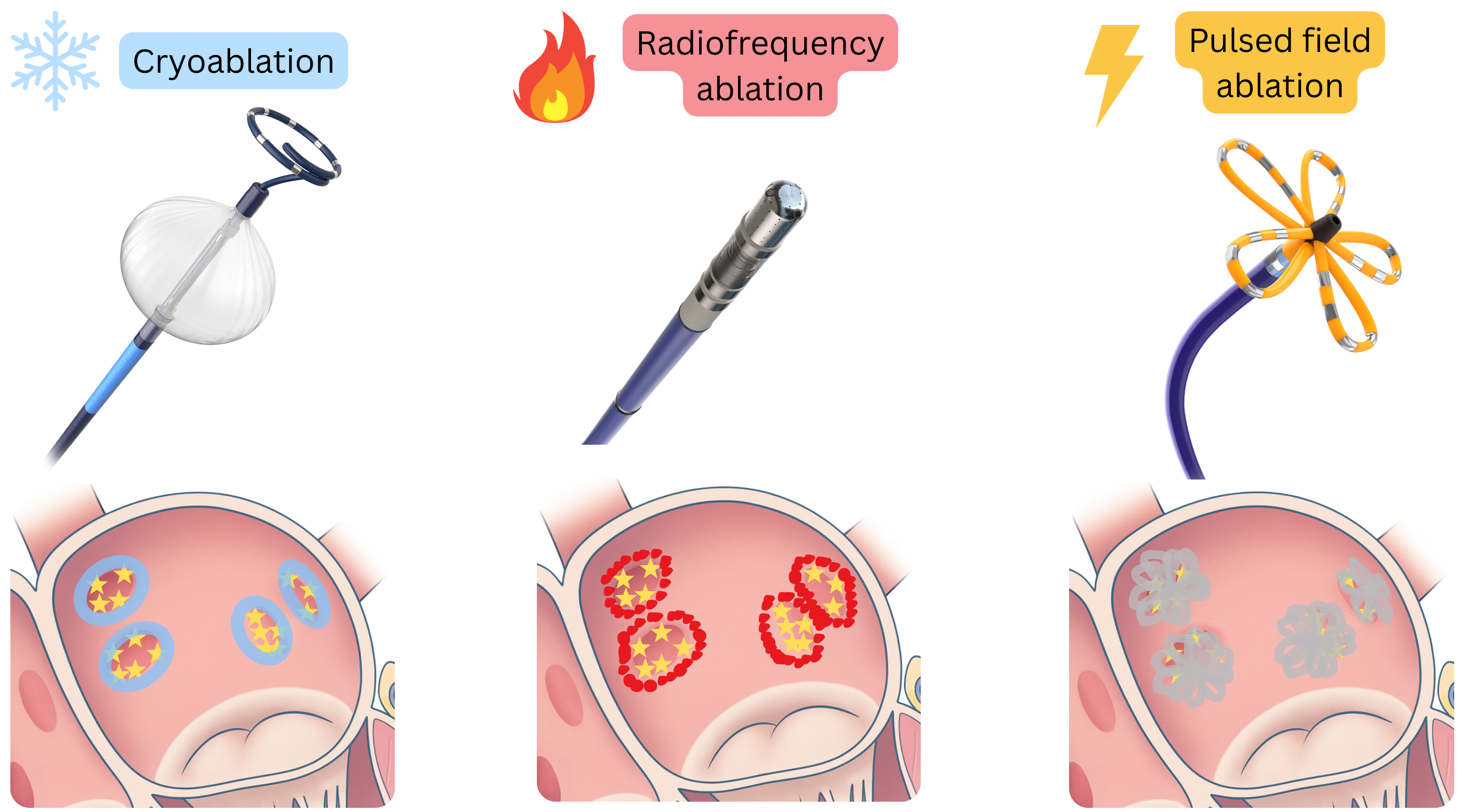
- In cardiology, three methods are used for ablation of atrial fibrillation (AF) and other arrhythmias:
- Radiofrequency ablation – myocardial destruction by heat
- Cryoablation – myocardial destruction by freezing
- Pulsed field ablation – myocardial destruction by electrical impulses
|
Atrial fibrillation ablation – methods (basic comparison)
|
| Radiofrequency ablation |
- Principle: The catheter tip is heated (~50 °C).
- Methodology: Lesions are created point by point around each pulmonary vein.
- Procedure time: 90–180 min.
- Complications: Atrio-oesophageal fistula, phrenic nerve injury, pulmonary vein stenosis.
|
| Cryoablation |
- Principle: The catheter has a balloon at its tip, which is advanced into the pulmonary vein at the ostium.
- Methodology: The balloon at the ostium of each vein is frozen (~ −50 °C).
- Procedure time: ~60 min.
- Complications: Phrenic nerve injury.
|
| Pulsed field ablation |
- Principle: The catheter is expanded at its distal end into a “sphere” or “flower” shape at the pulmonary vein ostium.
- Methodology: Electrodes on the catheter deliver short electrical impulses (electroporation).
- Procedure time: ~60 min.
- Complications: Minimal, virtually none.
|
AF ablation and pulmonary vein isolation
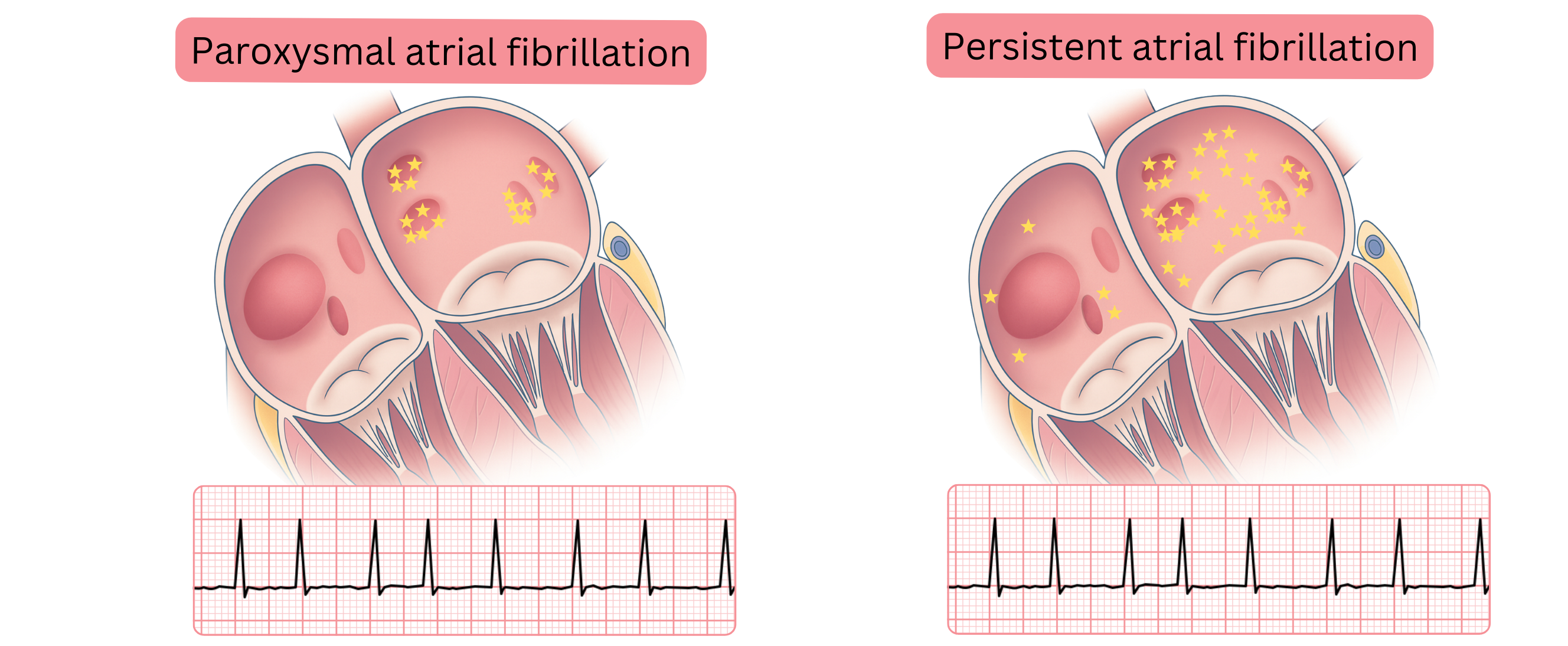
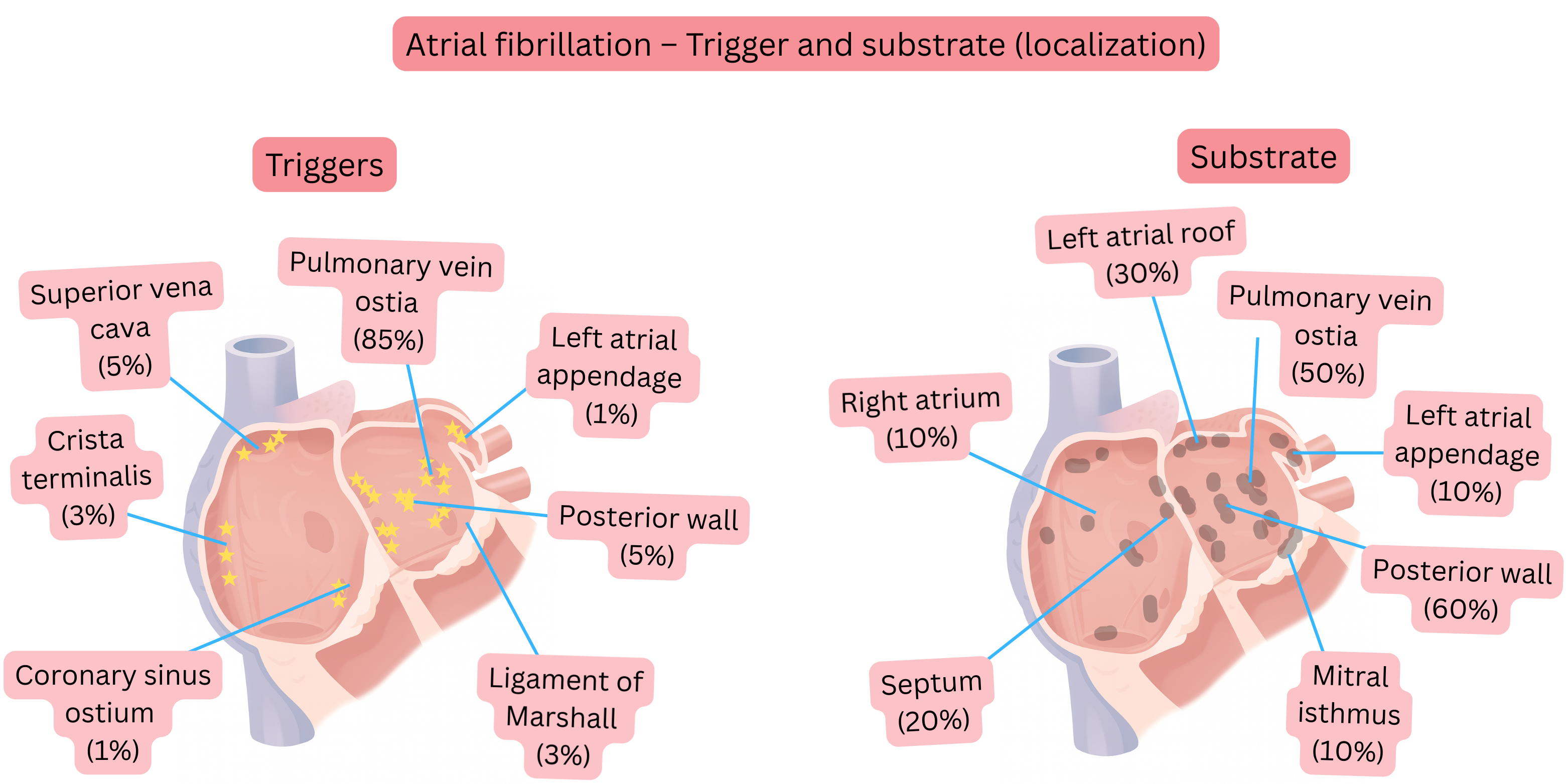
- AF initially presents as paroxysmal and originates (90%) in the region of the pulmonary vein ostia, where both the AF trigger and substrate are located in close proximity.
- Electrical impulses from the pulmonary vein ostia, from the activated substrate, propagate into the left atrium.
- Initially, this mechanism manifests clinically as paroxysmal AF.
- After several years, the substrate extends to other areas of the left atrium (roof, posterior wall, mitral isthmus).
- This expanded substrate manifests clinically as persistent AF.
- Pulmonary vein isolation (regardless of the method used) electrically isolates both the trigger and the substrate at the ostia.
- Therefore, pulmonary vein isolation is most effective in paroxysmal AF.
- If the substrate is also present outside the pulmonary vein ostia (persistent AF),
- more extensive ablation is performed (roof, posterior wall, mitral isthmus, superior vena cava).
Pulsed field ablation (basic procedure)
- Sheaths are inserted into the femoral veins in the groin (2 left, 1 right), through which catheters are advanced via the inferior vena cava into the right atrium:
- Left side: intracardiac echocardiography (ICE), catheter in the coronary sinus.
- Right side: transseptal puncture needle.
- Under ICE guidance, a transseptal puncture is performed through the fossa ovalis.
- Subsequently, the ablation catheter is advanced through the fossa ovalis into the left atrium.
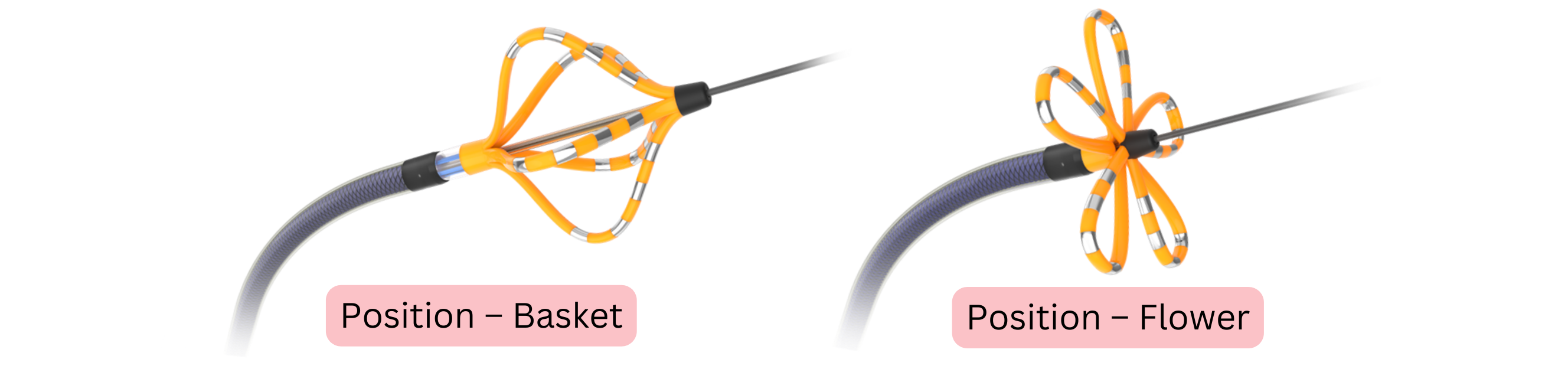
- A dedicated catheter is used for pulsed field ablation,
- which is deployed in the left atrium in a “flower” configuration with 5 splines,
- each spline contains 4 electrodes (positive and negative).
- During pulse delivery, a strong electric field is generated between the positive and negative electrodes,
- causing movement of ions and electrons between the electrodes.
- Particles pass through cardiomyocyte membranes and create pores,
- a process termed electroporation, leading to destruction of the myocardium and the arrhythmogenic substrate.
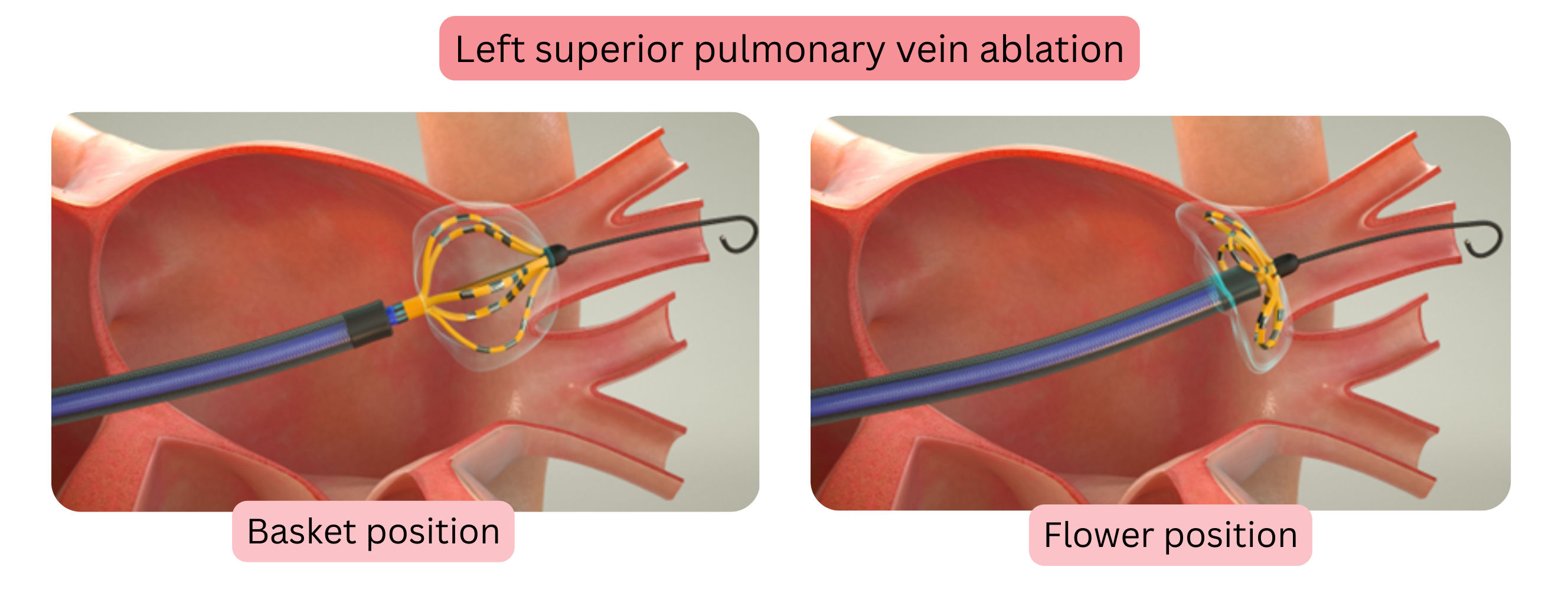
- The catheter is sequentially positioned in each pulmonary vein, first in the oval (basket) configuration and subsequently in the “flower” configuration.
- Electrical pulses are delivered in both configurations.
- Pulsed field ablation is cardioselective:
- it induces irreversible electroporation of cardiomyocytes and the arrhythmogenic substrate,
- surrounding tissues (vessels, nerves, oesophagus) remain unaffected.
| Atrial fibrillation ablation |
Class |
| Pulsed field ablation (not radiofrequency or cryoablation) is recommended as the preferred method of atrial fibrillation ablation. |
I |

