
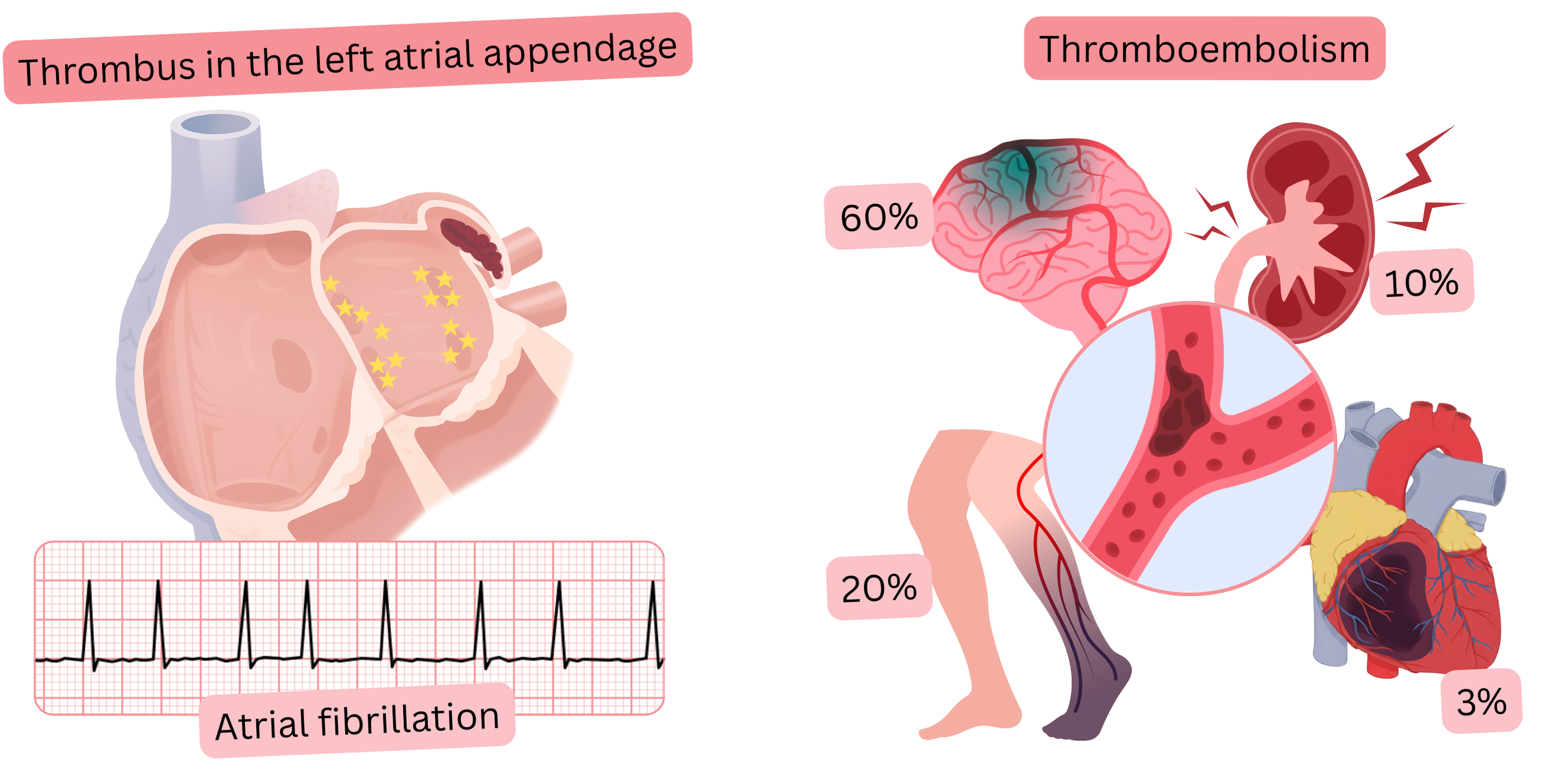
Thromboembolism is a condition in which a thrombus detaches from its site of origin, circulates in the bloodstream as an embolus, and subsequently causes an embolism (occlusion or stenosis of a vessel) at another site in the body.
Atrial fibrillation (AF) is one of the major risk factors for thromboembolism, which in AF most commonly manifests as embolic ischemic stroke (IS).
The risk of ischemic stroke in AF (without anticoagulant therapy) can be calculated using the CHA2DS2-VA score.
When estimating thromboembolic risk, the diagnosis of “atrial fibrillation” is essential,
Risk of thromboembolism in AF without anticoagulant therapy
| Thromboembolism and Atrial Fibrillation | ||
|---|---|---|
| Site of embolization | Prevalence | Clinical manifestation |
| Cerebral arteries | 50 – 70 % |
Ischemic stroke (IS) Transient ischemic attack (TIA) |
| Arteries of the lower extremities | 15 – 25 % | Ischemia and gangrene of the lower extremities |
| Renal arteries | 10 – 15 % |
Lumbar pain Hematuria Arterial hypertension Acute kidney injury |
| Mesenteric artery | 5 – 10 % |
Abdominal pain Nausea Vomiting |
| Coronary arteries | < 5 % |
Angina pectoris Myocardial infarction (STEMI, NSTEMI) |
20% of all ischemic strokes are caused by thromboembolism in AF.
For prevention of thromboembolism, anticoagulant therapy is recommended, not antiplatelet therapy.
There are several scoring systems,
Scoring systems use comorbidities and risk factors associated with AF, for example:
The best-known scoring systems include:
Each scoring system uses different parameters, but most agree:
| Thromboembolic risk and atrial fibrillation | Class |
|---|---|
| Atrial fibrillation is one of the major risk factors for thromboembolism, regardless of whether AF is paroxysmal, persistent, permanent, symptomatic, or asymptomatic. | I |
| Annual thromboembolic risk in % is estimated using the CHA2DS2-VASc score or the newer CHA2DS2-VA score (since 2024). | I |
| For prevention of thromboembolism in atrial fibrillation, anticoagulant therapy (not antiplatelet therapy) is recommended. | I |
| Antiplatelet therapy (Aspirin, Clopidogrel) is not recommended for prevention of thromboembolism in atrial fibrillation. | III |
The following table shows the risk of thromboembolism according to the CHA₂DS₂-VASc score,
| CHA₂DS₂-VASc score and risk of thromboembolism (1 year) | ||
|---|---|---|
| CHA₂DS₂-VASc | Ischemic stroke | Ischemic stroke/TIA/systemic embolism |
| 0 | 0,2 % | 0,3 % |
| 1 | 0,6 % | 0,9 % |
| 2 | 2,2 % | 2,9 % |
| 3 | 3,2 % | 4,6 % |
| 4 | 4,8 % | 6,7 % |
| 5 | 7,2 % | 10,0 % |
| 6 | 9,7 % | 13,6 % |
| 7 | 11,2 % | 15,7 % |
| 8 | 10,8 % | 15,2 % |
| 9 | 12,2 % | 17,4 % |
IS – Ischemic stroke. TIA – Transient ischemic attack.
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
