
An accessory pathway is present in 0.1–0.3 % of the population.
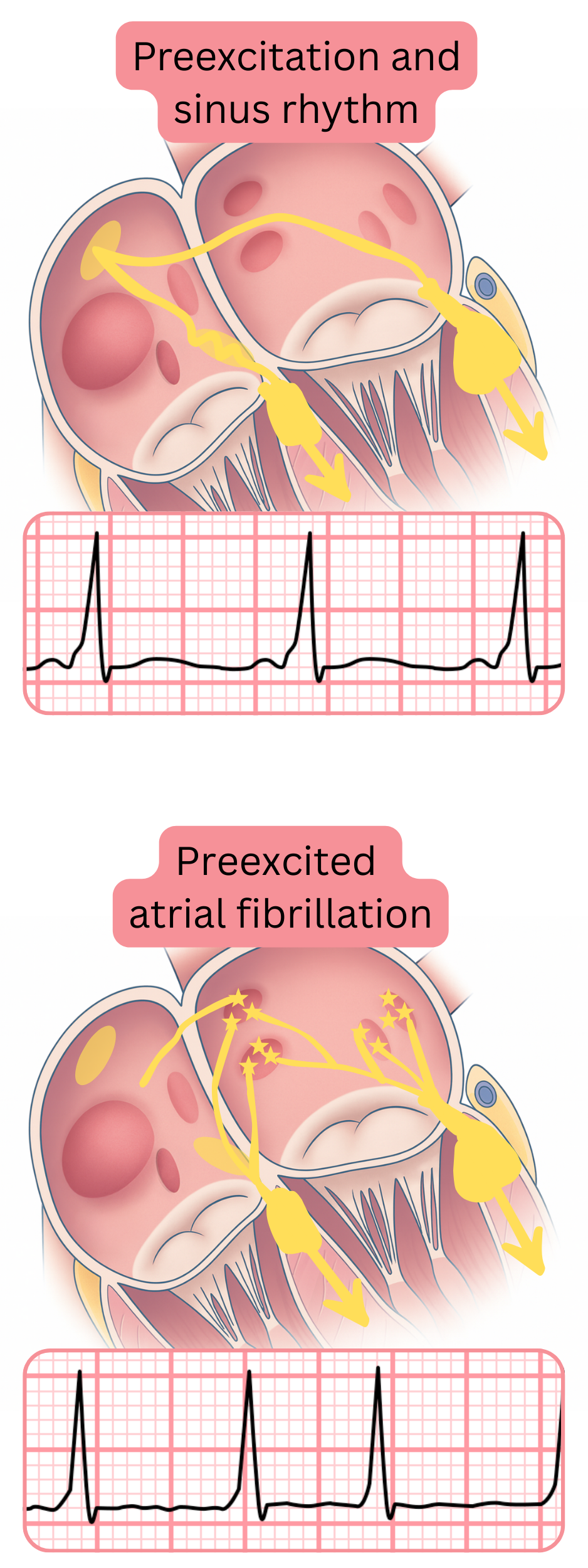
An accessory pathway (anterograde) produces pre-excitation. Pre-excitation means that part of the ventricles is activated (excited) earlier than via the conduction system (AV node -> His -> bundle branches). Pre-excitation produces a delta wave on ECG.
WPW syndrome (symptomatic pre-excitation)
WPW pattern (asymptomatic pre-excitation)
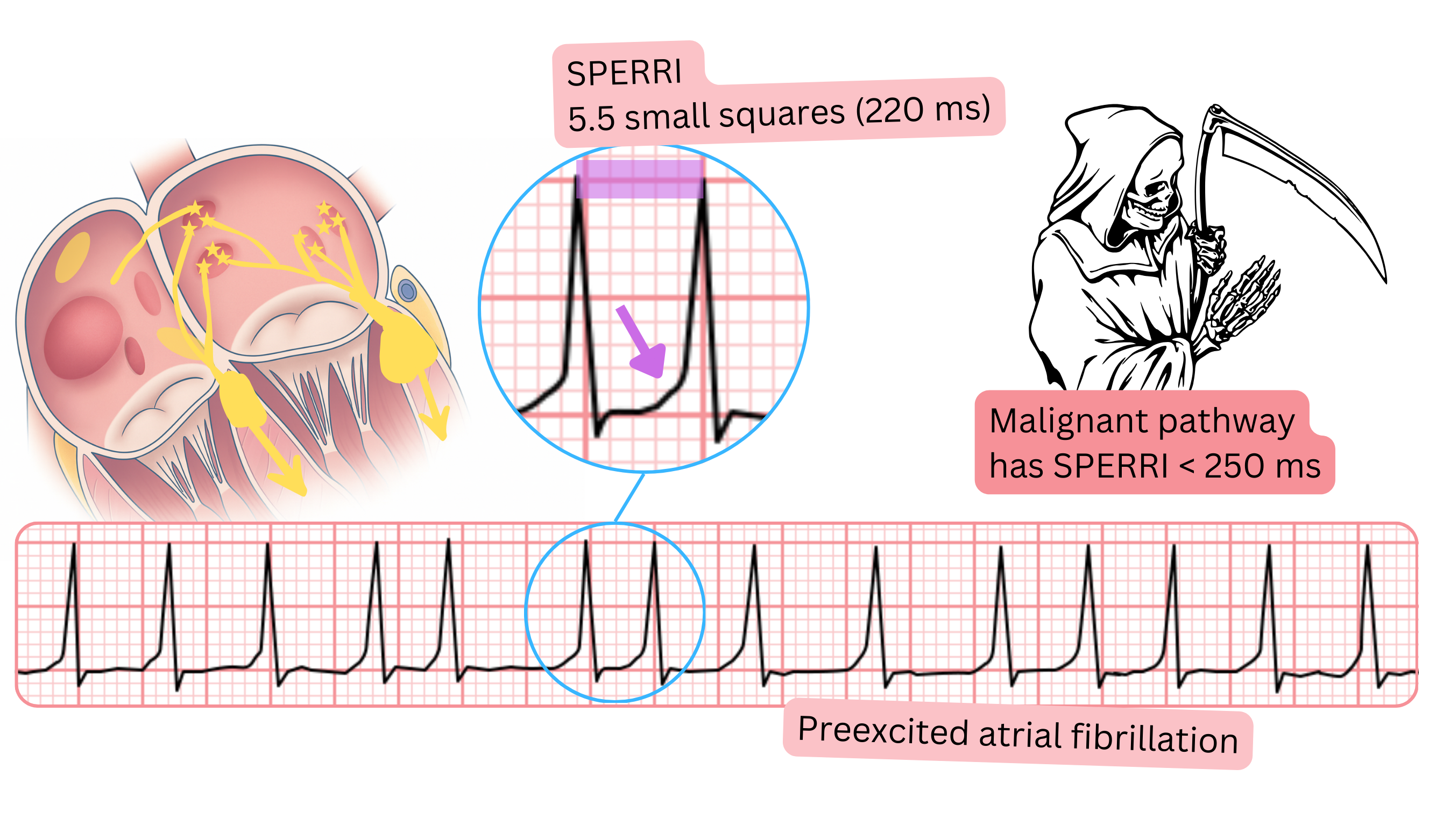
Malignant accessory pathway
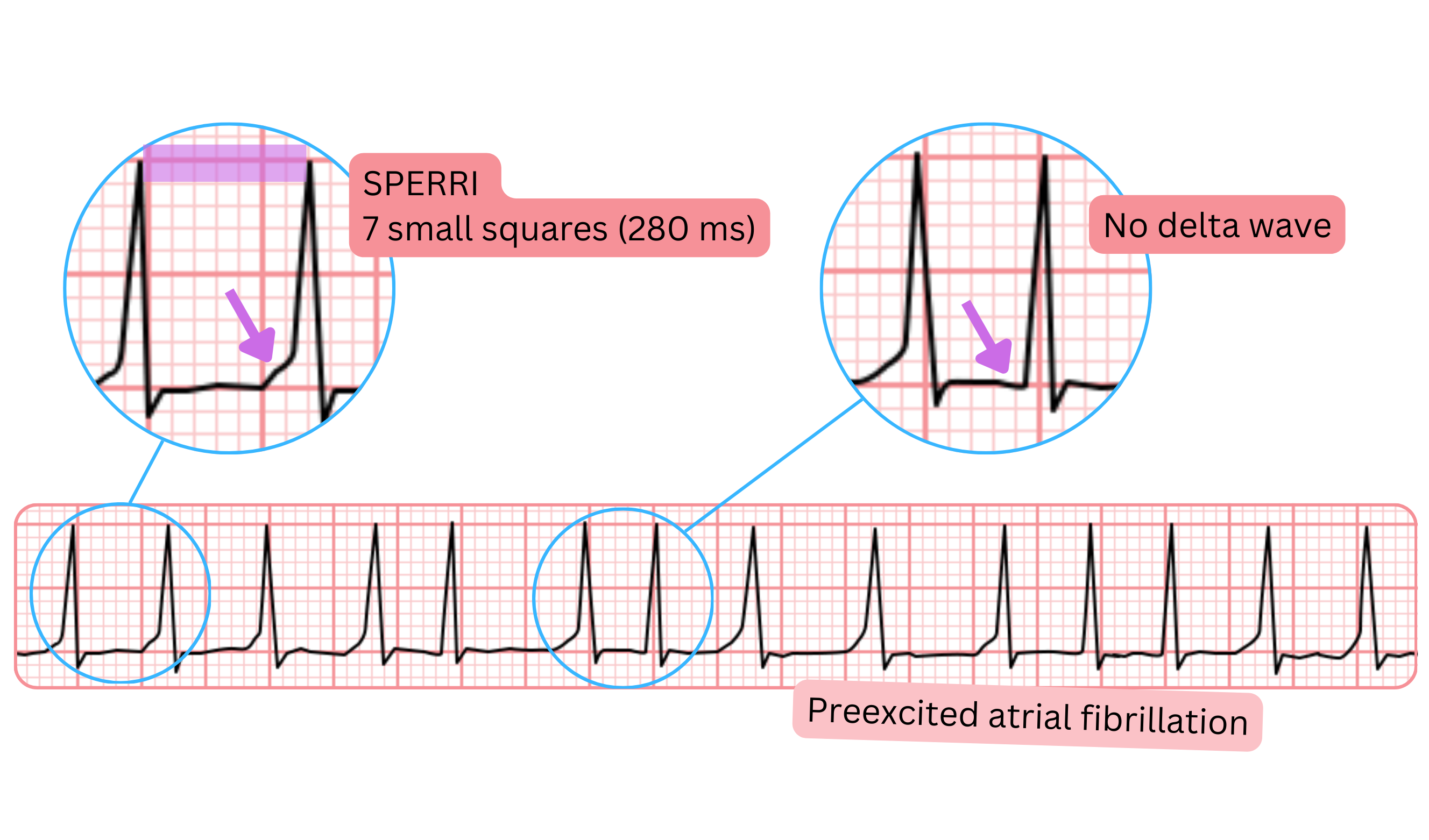
SPERRI (Shortest Preexcited RR Interval)
| Accessory pathway and atrial fibrillation | Class |
|---|---|
| For treatment of WPW syndrome, catheter ablation of the accessory pathway is recommended. | I |
| A malignant accessory pathway is defined as the shortest RR interval ≤250 ms with a delta wave (SPERRI ≤250 ms) during AF. | I |
| For treatment of a malignant accessory pathway, catheter ablation of the accessory pathway is recommended. | I |
| Ablation of the accessory pathway should be considered if SPERRI ≤300 ms. | IIa |
In pre-excited AF, the following are contraindicated:
|
III |
In hemodynamically stable pre-excited AF, the following are recommended:
|
I |
| In hemodynamically unstable pre-excited AF, electrical cardioversion is recommended. | I |
In pre-excited AF (AF + delta wave), all drugs that slow conduction through the AV node and do not block the accessory pathway are contraindicated. If the patient receives these drugs, ventricular fibrillation may occur. Contraindicated drugs include:
| In pre-excited atrial fibrillation, the following may be administered |
|---|
| Procainamide |
| Ibutilide |
| Flecainide |
| Electrical cardioversion |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
