
The prevalence of atrial fibrillation (AF) in the general population is 2–4 %.
The prevalence of AF increases with age. AF affects
| Prevalence of atrial fibrillation and age | |
|---|---|
| AF prevalence | Age |
| 2 % | <65 years |
| 9 % | >65 years |
The aim of screening is to diagnose AF at a stage when AF is asymptomatic, or when the patient has non-specific symptoms: weakness, fatigue, vertigo, etc.
AF begins as paroxysmal episodes that are triggered by atrial arrhythmias originating from the region of the pulmonary vein ostia. These initial AF paroxysms terminate spontaneously within 24 h, and in 30–50 % of patients they are asymptomatic or present with non-specific symptoms: weakness, fatigue, vertigo, etc.
10 % of patients have silent AF, which carries the highest risk of thromboembolism (particularly stroke). These patients are unaware that they have AF and therefore do not receive anticoagulation therapy according to the CHA2DS2-VA score.
In clinical practice, the terms asymptomatic and silent AF are often confused:
| Silent atrial fibrillation |
|---|
| 10 % of patients have silent AF. Patients have no symptoms and are unaware that they have AF. |
| 30–50 % of patients in the early stage of AF during paroxysms are asymptomatic or have non-specific symptoms (weakness, fatigue, vertigo). |
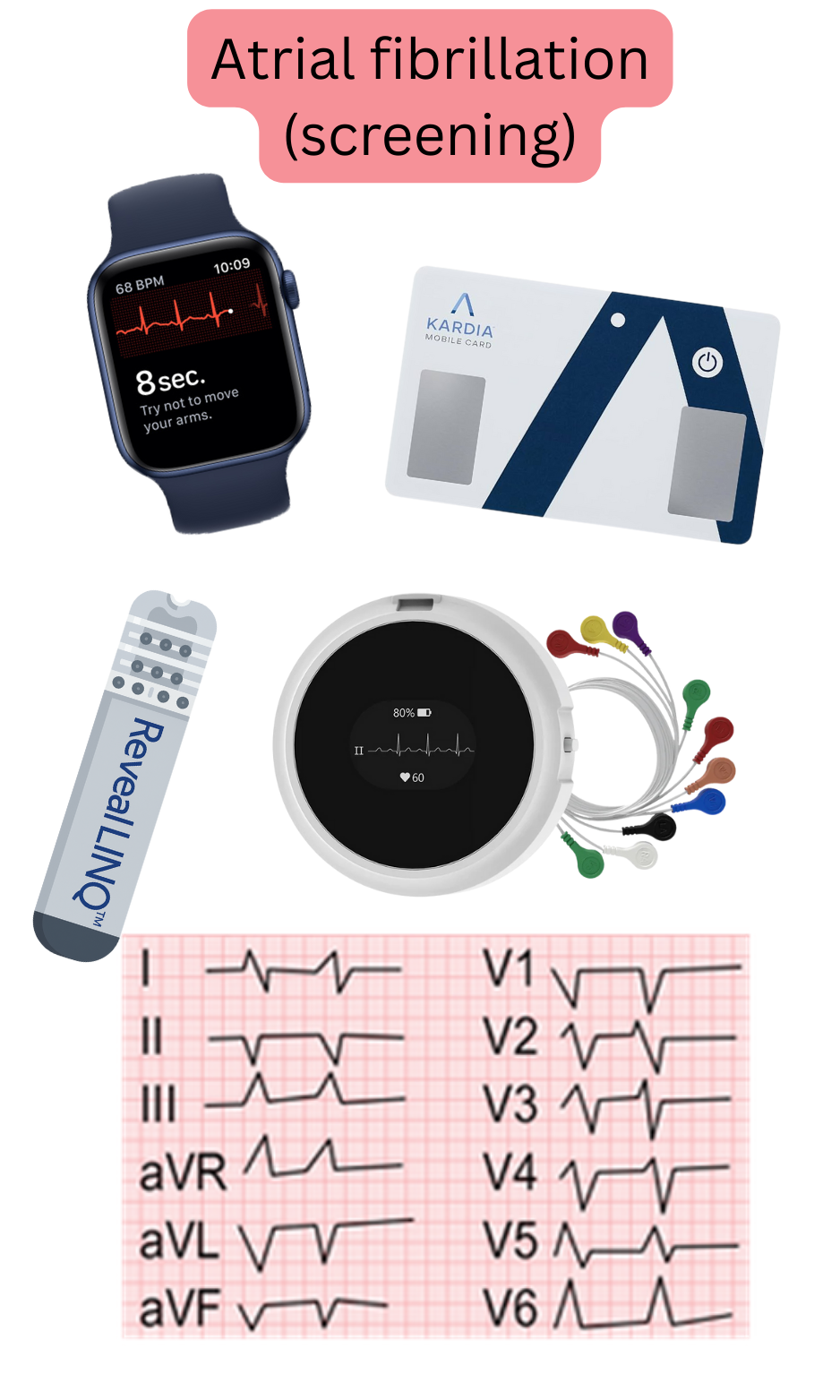
For AF screening, any device that records the electrical activity of the heart based on the voltmeter principle and displays this activity as an ECG tracing is recommended:
A major advantage of smart devices with ECG is that patients carry them at all times (ECG watches). The patient can therefore record an ECG during symptoms (palpitations, etc.), which may occur, for example, once per month.
When AF is detected using smart devices with ECG, the patient must immediately contact a physician for comprehensive evaluation and initiation of anticoagulation therapy according to the CHA2DS2-VA score.
| Screening for atrial fibrillation and devices | Class |
|---|---|
|
For AF screening, any device capable of recording an ECG is recommended:
|
I |
|
For AF screening, devices that do not record an ECG may be considered:
|
IIb |
| The diagnosis of atrial fibrillation based on ECG must be confirmed by a physician in an outpatient setting, or online via a trusted platform, e.g. www.ECGsmart.com | I |
Investigations or devices that do not record an ECG should not be used for AF screening:
Photoplethysmography (PPG) is pulse measurement using light. The device continuously emits light (most commonly green), which is reflected from the pulsating artery. The device then detects the reflected light and determines the pulse rate. Devices that measure pulse based on PPG include smart watches, bands, or an oximeter.
The main limitation of atrial fibrillation screening is that the patient may not experience an AF episode at the time the ECG is recorded. The most effective AF screening method would be implantation of a loop recorder; however, this is not routinely performed because it is an invasive procedure associated with risks (infection, haematoma) and would be financially demanding.
Implantation of a loop recorder is indicated in patients after ESUS (Embolic Stroke of Undetermined Source).
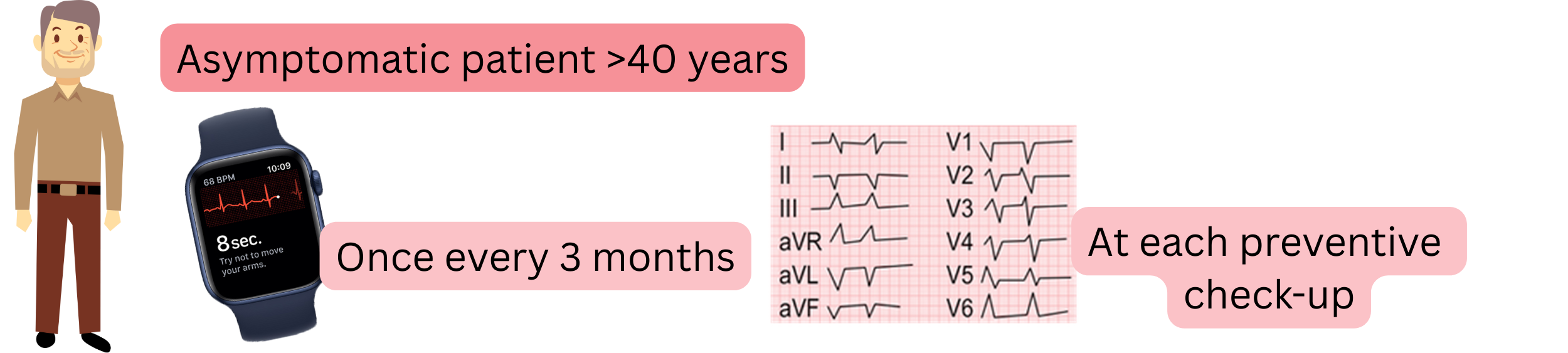
| Screening for atrial fibrillation in asymptomatic patients (>40 years) | Class |
|---|---|
| It is recommended to record an ECG using a smart device with ECG (ECG watch, blood pressure monitor with ECG, ECG card) once every 3 months. | I |
| It is recommended to record an ECG at every preventive medical examination. | I |
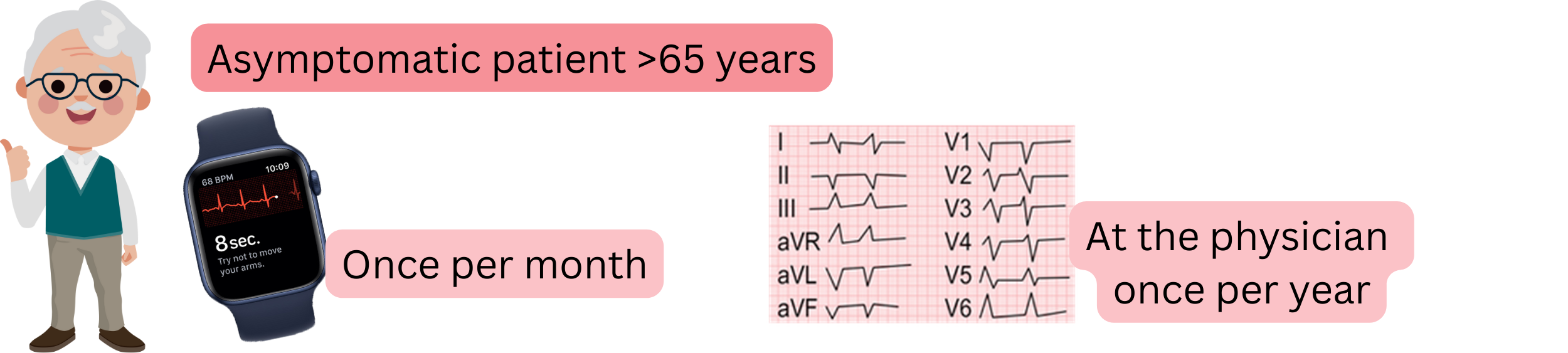
| Screening for atrial fibrillation in asymptomatic patients (>65 years) | Class |
|---|---|
| It is recommended to record an ECG using a smart device with ECG (ECG watch, blood pressure monitor with ECG, ECG card) once per month. | I |
| It is recommended to record an ECG at the physician’s office once per year. | I |
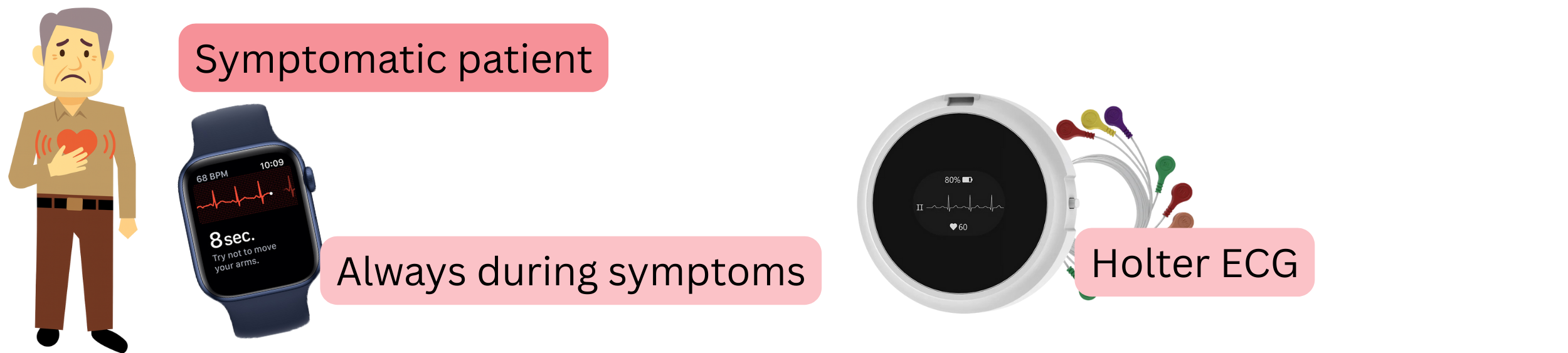
| Screening for atrial fibrillation in symptomatic patients | Class |
|---|---|
| During symptoms (specific or non-specific), it is recommended to immediately record an ECG using a smart device with ECG (ECG watch, blood pressure monitor with ECG, ECG card). | I |
| ECG Holter monitoring is recommended: 24-hour or 7-day (preferably). | I |
| Screening for atrial fibrillation in patients after ESUS (Embolic Stroke of Undetermined Source) | Class |
|---|---|
| Implantation of a loop recorder is recommended. | I |
| During symptoms (specific or non-specific), it is recommended to immediately record an ECG using a smart device with ECG (ECG watch, blood pressure monitor with ECG, ECG card). | I |
| ECG Holter monitoring (24-hour or 7-day, preferably) may be considered. | IIa |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
