
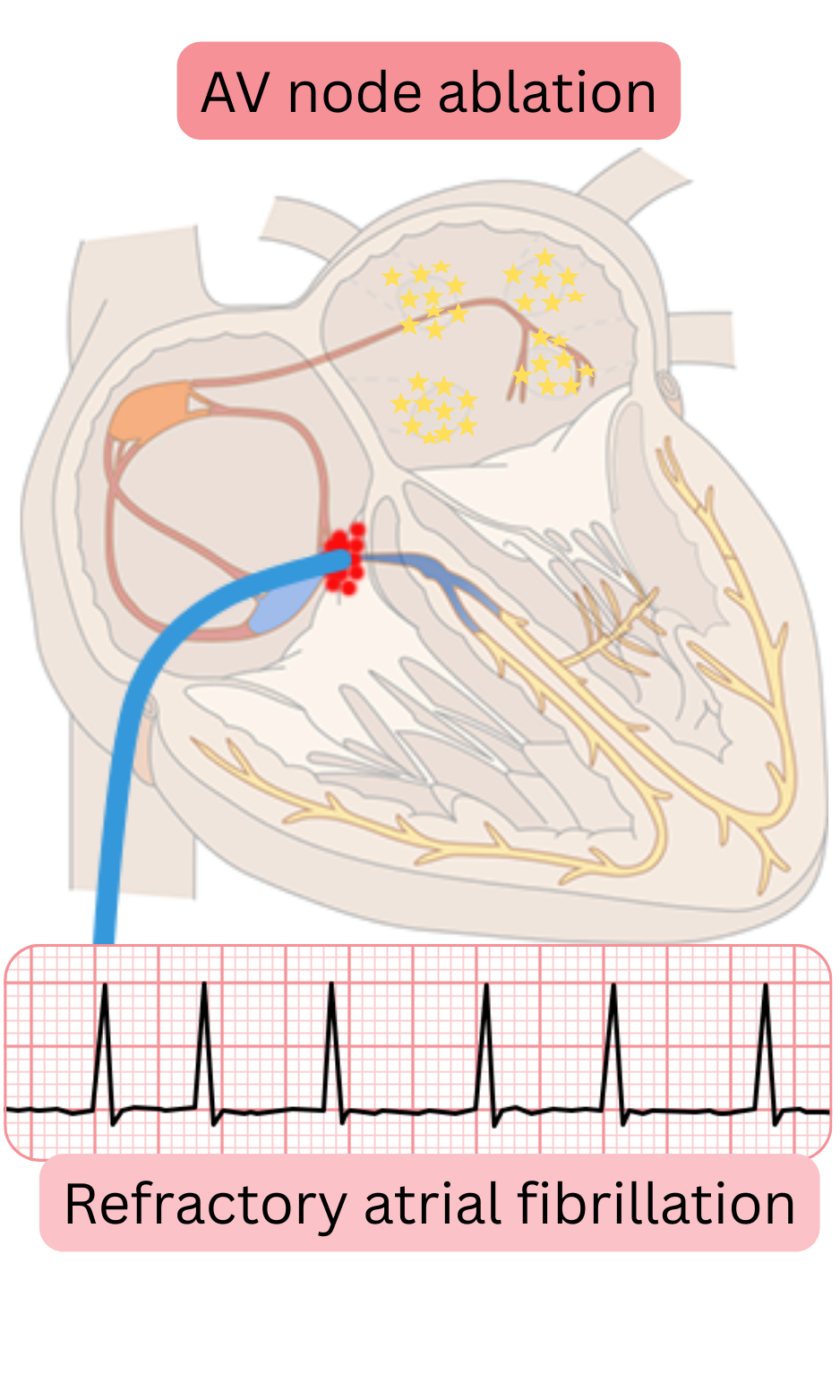
Pace and ablate treatment of atrial fibrillation (AF) is:
Refractory AF is a condition,
when symptoms persist and/or ventricular rate is inadequate (>100/min) and the following conditions have been met:
| Refractory atrial fibrillation | |
|---|---|
| Definition | Persistent symptoms and/or inadequate ventricular rate > 100/min |
| Reversible causes | Excluded (hypertension, thyrotoxicosis, obesity, alcohol, stress, etc.) |
| Pharmacological therapy | Failure (≥ 1 class I or III anti-arrhythmic drug and rate-control drugs) |
| Catheter ablation | Unsuccessful ablation (≥ 2 attempts of pulsed field ablation) |
| Symptoms | Persist |
The pace and ablate strategy is the last treatment option for refractory AF.
The indication for the “pace and ablate” strategy is refractory AF.
The goal of the “Pace and Ablate” strategy is to:
In asymptomatic persistent AF, rate control may be chosen after discussion with the patient.
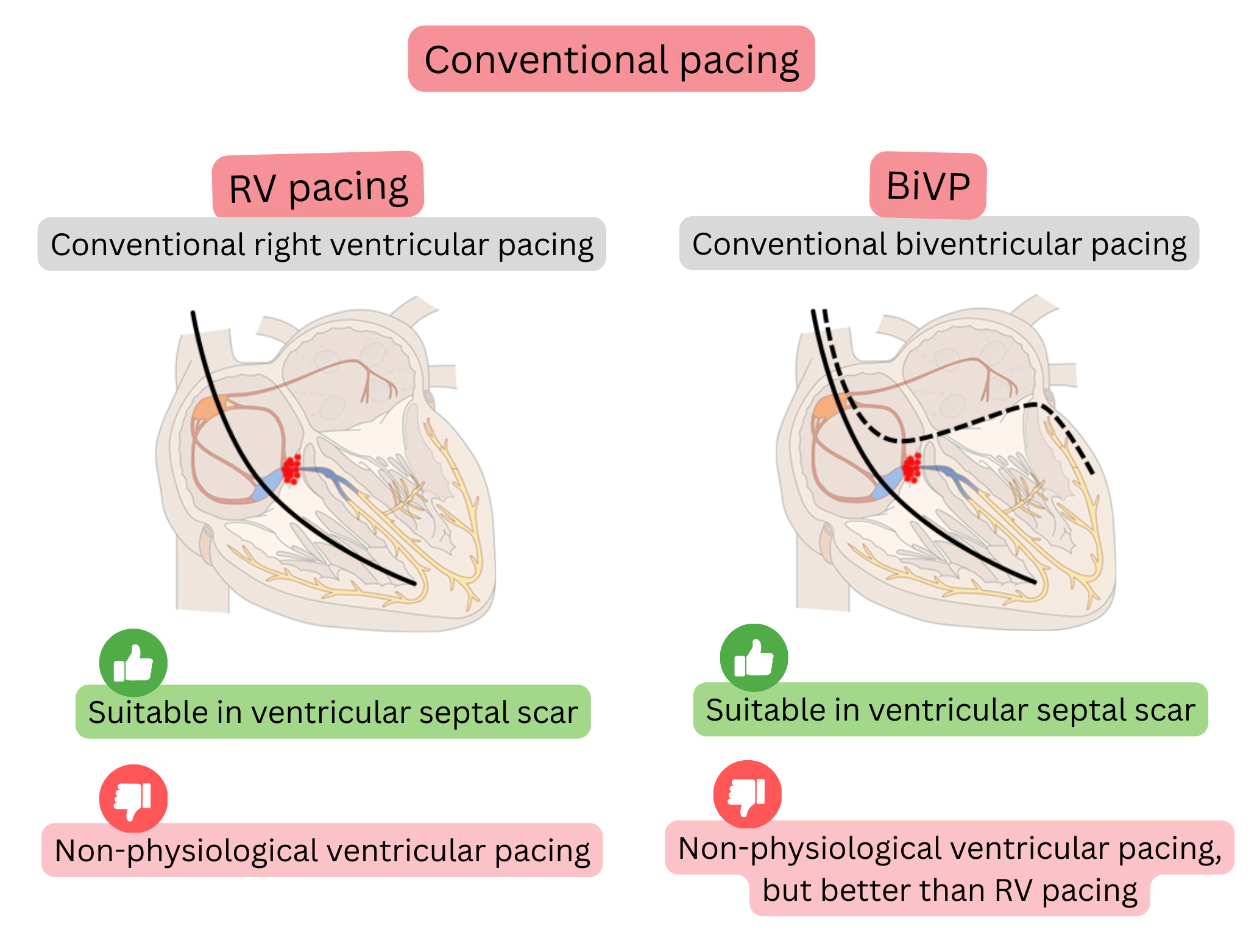
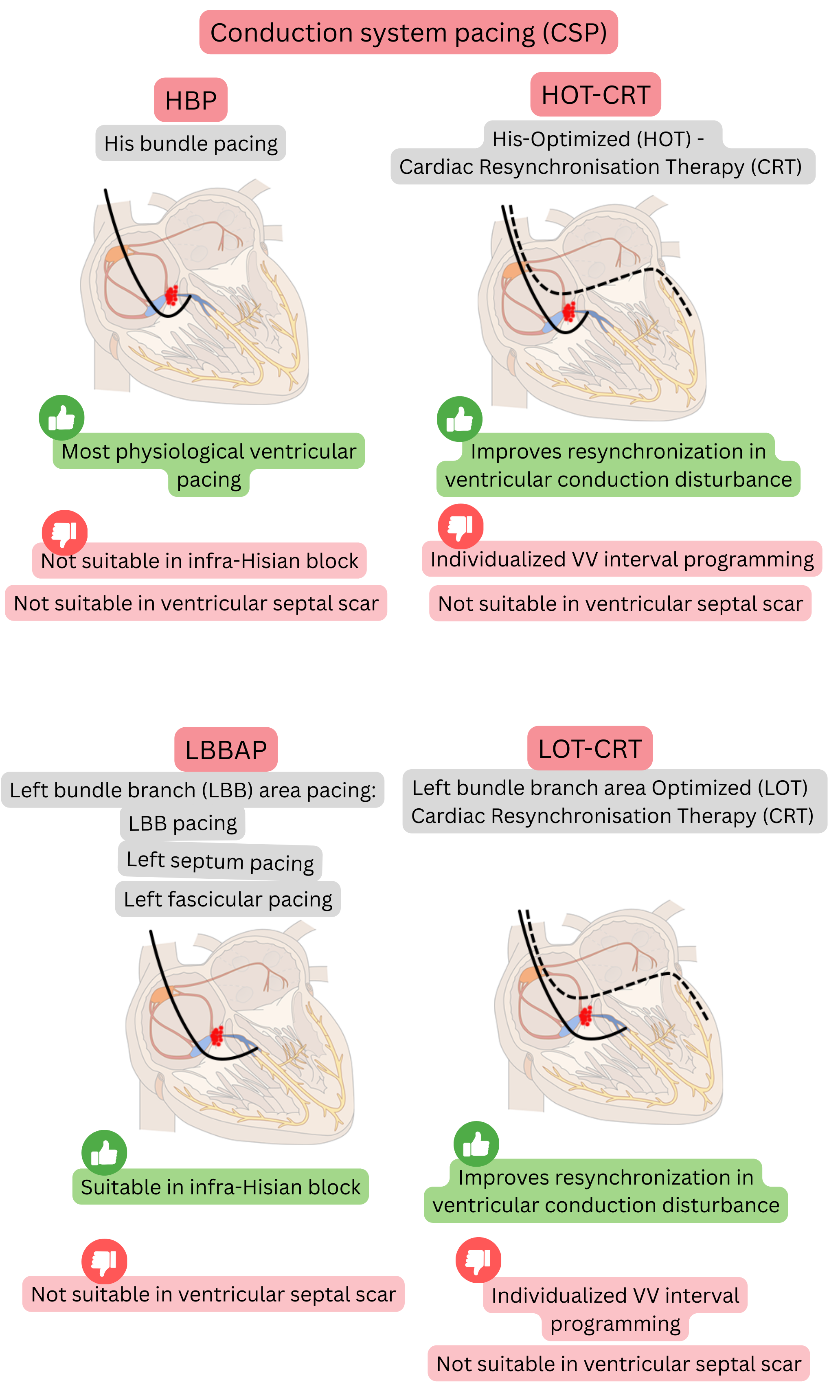
After pacemaker implantation, the goal is to achieve ventricular synchrony and avoid pacing-induced cardiomyopathy. Ventricular pacing modalities include:
In the “Pace and Ablate” strategy for AF, conduction system pacing (HBP or LBBAP) is preferred.
| Pace and Ablate strategy for atrial fibrillation treatment | Class |
|---|---|
The Pace and Ablate strategy for AF may be considered if AF is symptomatic and the following have failed:
|
IIa |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
