
Digoxin does not bind directly to cardiac receptors but stimulates the vagus nerve,
Classification:

Mechanism:
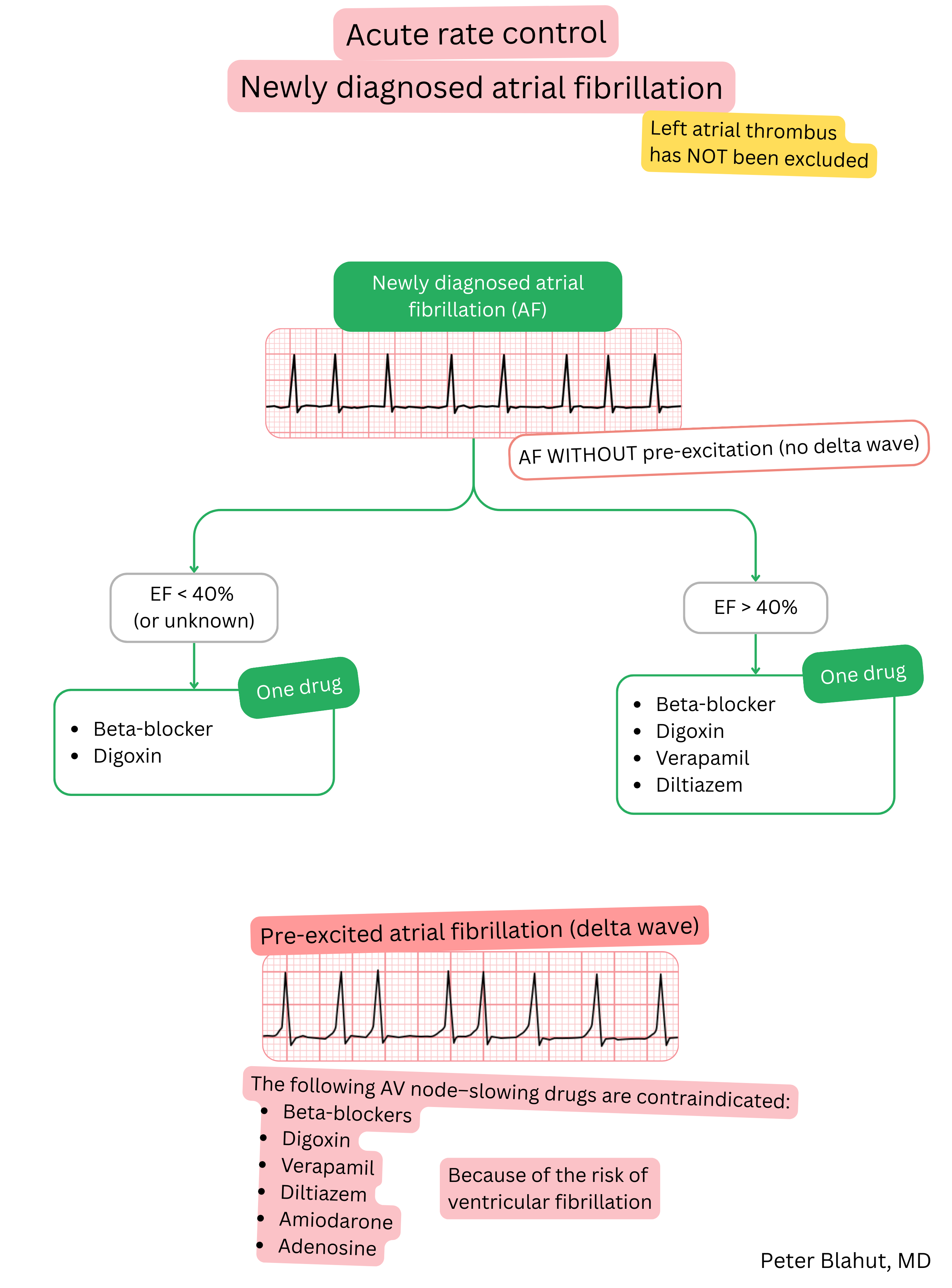
Effect on AF:
| Digoxin and atrial fibrillation (AF) |
|---|
| Brand names |
| Digoxin, Lanoxin, Lanicor, Lanacordin |
| Indications |
|
| Dosing |
|
| Onset of action |
|
| Effect |
|
| Duration of action |
|
| Therapeutic serum level |
|
| Contraindications |
|
Patient monitoring after initiation of digoxin:
| Patient monitoring after initiation of digoxin | ||
|---|---|---|
| Time since initiation | What to monitor | Reason for treatment interruption |
| Week 1 |
ECG Heart rate Potassium level (K⁺) Serum digoxin level |
Bradycardia < 50/min. AV block II or III degree Serum digoxin level > 2.0 ng/ml Hypokalaemia |
| Month 1 |
ECG Heart rate Potassium level (K⁺) Serum digoxin level |
Bradycardia < 50/min. AV block II or III degree Serum digoxin level > 2.0 ng/ml Hypokalaemia Inadequate clinical response |
| 6–12 months |
ECG Heart rate Potassium level (K⁺) Serum digoxin level |
Bradycardia < 50/min. AV block II or III degree Serum digoxin level > 2.0 ng/ml Hypokalaemia Inadequate clinical response |
Adverse effects:
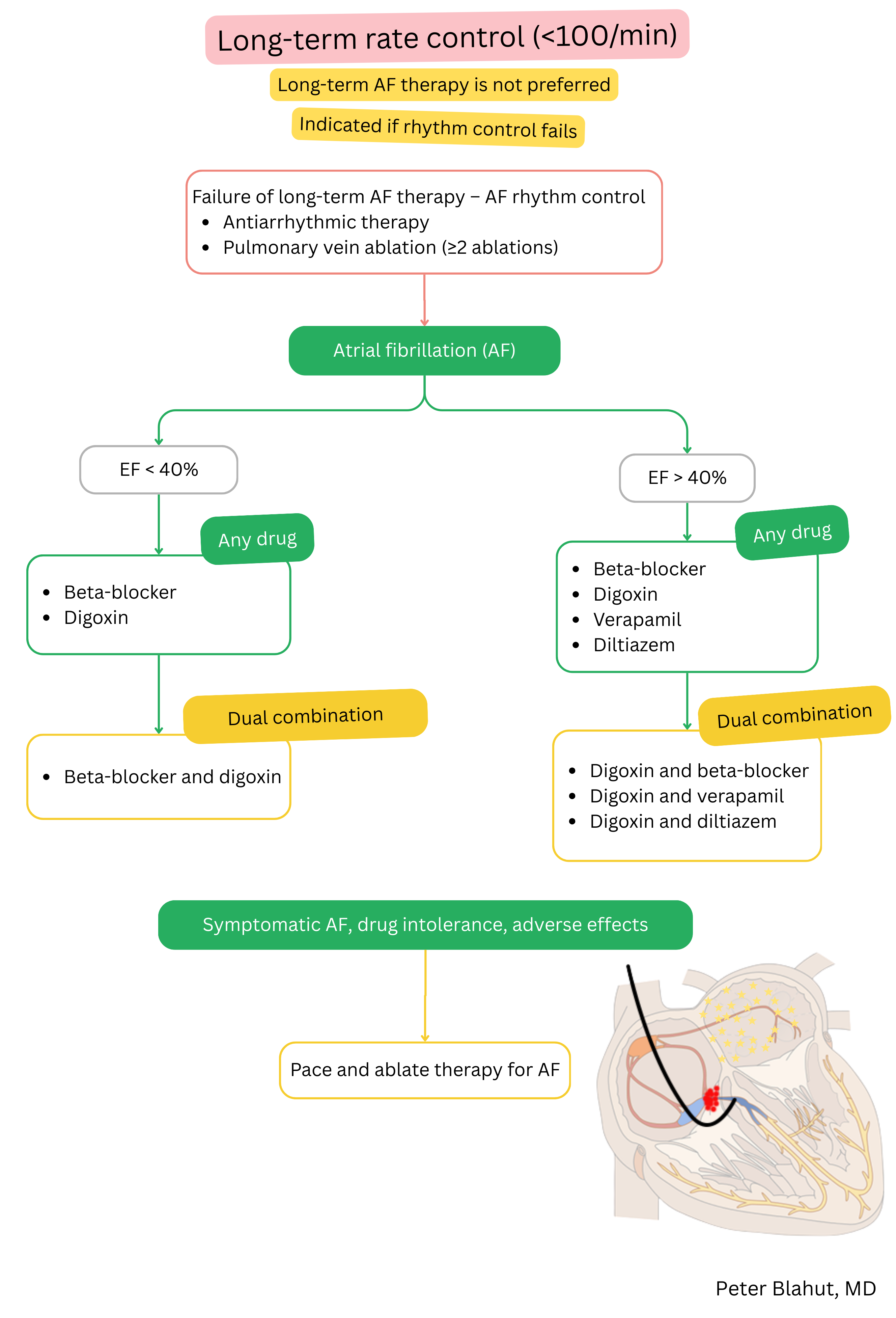
Digoxin and beta-blockers are used for ventricular rate control in AF (not for maintenance of sinus rhythm).
| Digoxin vs. beta-blockers in atrial fibrillation (AF) | ||
|---|---|---|
| Characteristic | Digoxin | Beta-blockers |
| Preferred patients | Sedentary patients with ejection fraction < 40 % | Most patients – especially with coronary artery disease and chronic stress |
| Effect | Slows rate mainly at rest | Slow rate at rest and during exertion |
| Use | Often as add-on therapy to beta-blockers or non-DHP calcium channel blockers | First-line drug for rate control |
| Limitations | Limited effect during exertion, risk of toxicity | Caution in bradycardia, asthma/COPD, hypotension |
| Adverse effects | Nausea, vomiting, arrhythmias (AV block, ventricular tachyarrhythmias), visual disturbances (xanthopsia) | Bradycardia, hypotension, fatigue, bronchospasm, worsening HF in decompensated patients |
CAD – coronary artery disease, BB – beta-blockers, non-DHP CCB – non-dihydropyridine calcium channel blockers
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
