Atrial flutter (AFl) shares the same risk factors as atrial fibrillation (AF). In remodelled atria, most commonly in the right atrium, a re-entry circuit develops along which the electrical impulse can circulate, most commonly at a rate of 240–300/min.
For the impulse to start circulating within a re-entry circuit, a trigger is required; the most common triggers are:
- atrial premature beat
- AF (short episode)
20 % of patients with AF also have AFl (typical or atypical).
In 50 % of patients with AFl, AF develops in the future.
The thromboembolic risk in AFl is the same as in AF:
- therefore, anticoagulation therapy in AFl is initiated as in AF, according to the CHA2DS2-VA score.
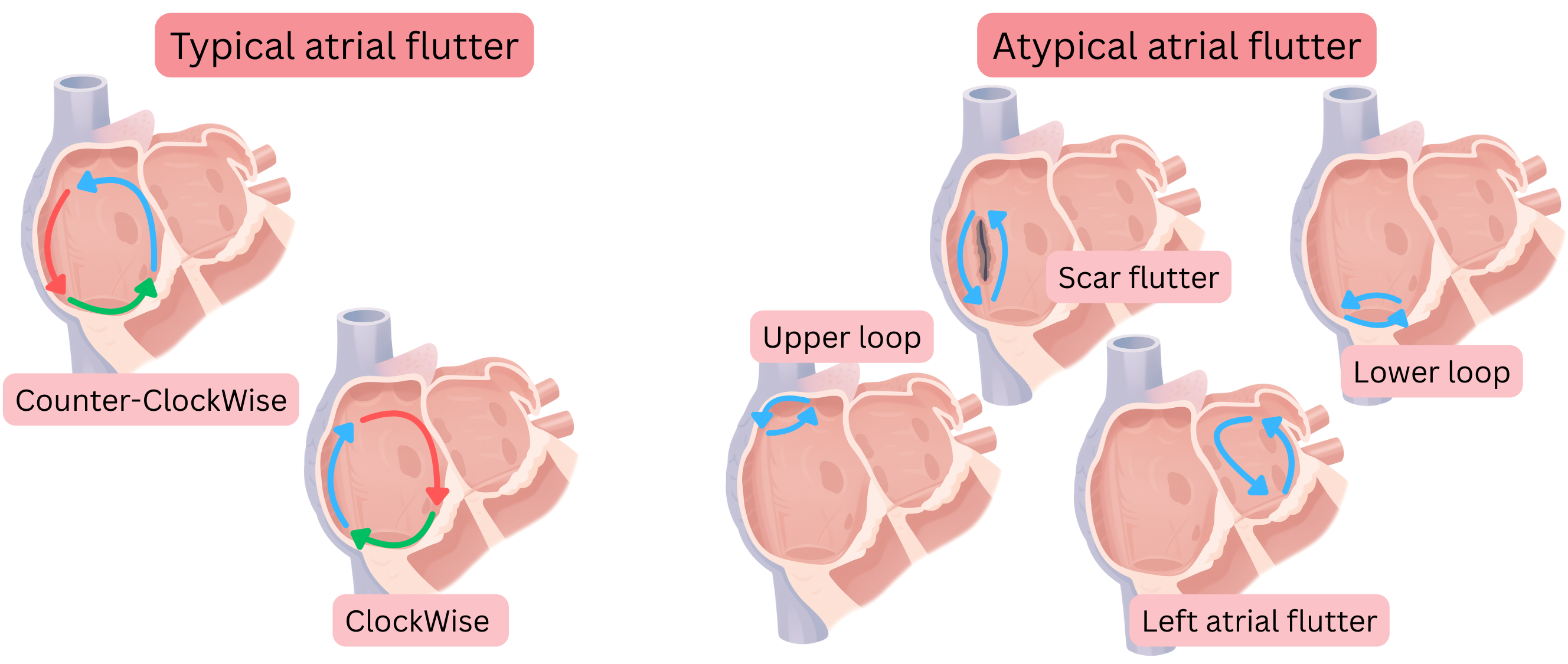
AFl is classified according to the location of the re-entry circuit and the direction of impulse rotation into:
- Typical AFl
- CCW typical AFl (Counter-Clockwise AFl)
- CW typical AFl (Clockwise AFl)
- Atypical AFl
AFl is present in 1 % of the population, of which:
- CCW typical AFl (80 %)
- CW typical AFl (10 %)
- Atypical AFl (10 %)
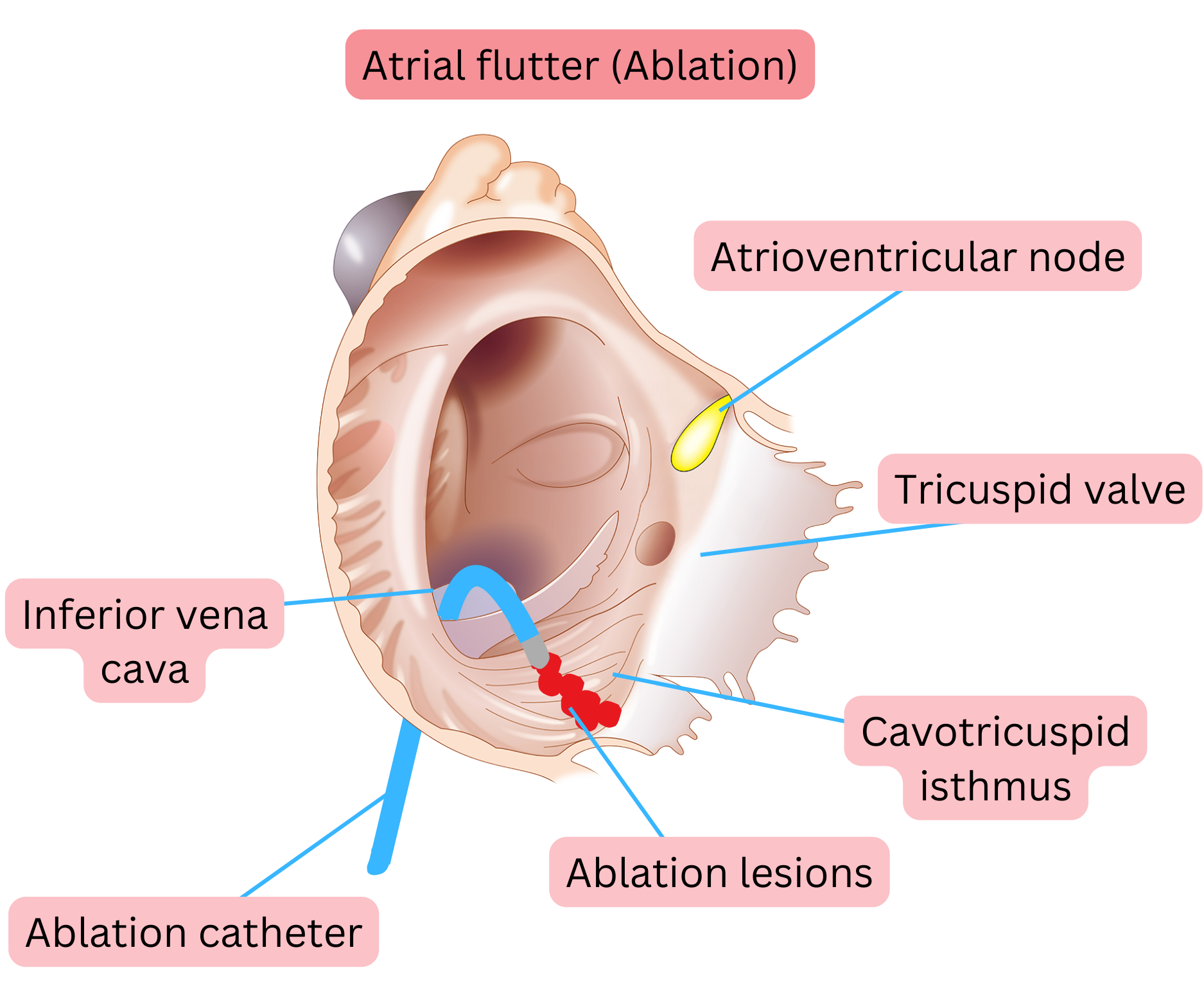
Typical AFl means that the re-entry circuit is located in the right atrium and proceeds as follows:
- Down the free wall of the right atrium (anterior to the crista terminalis)
- Through the cavotricuspid isthmus (CTI)
- Up through the atrial septum
- Then across the roof of the right atrium back to the free wall of the right atrium.
- The diameter of the re-entry is approximately 3 cm, corresponding to a re-entry path length of approximately 9 cm.
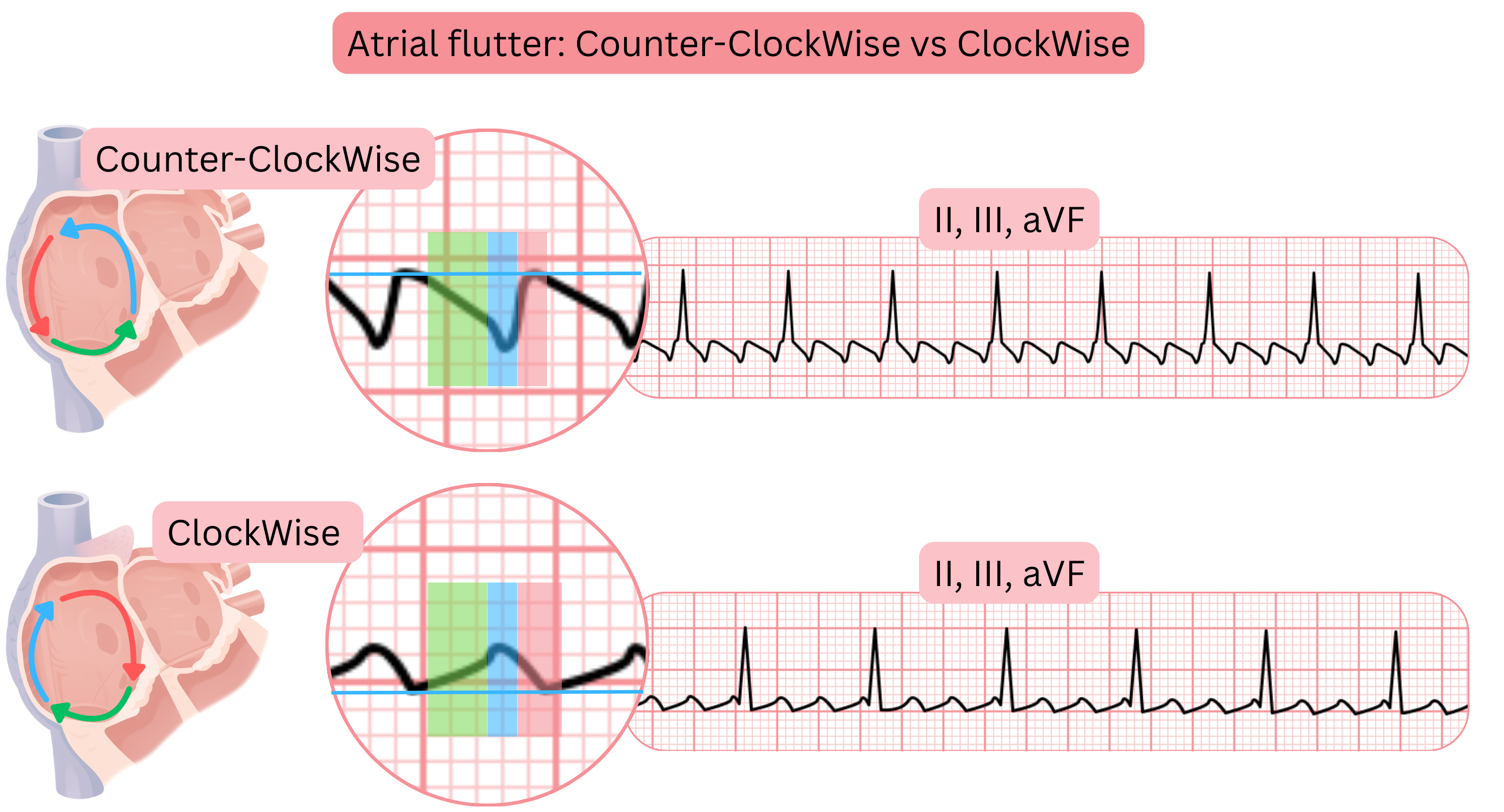
- Depending on the direction of impulse rotation within the re-entry circuit, typical AFl is divided into:
- CCW AFl (Counter-Clockwise)
- the impulse rotates counter-clockwise
- CW AFl (Clockwise)
- the impulse rotates clockwise
Atypical AFl means that the re-entry circuit differs from that of typical AFl.
- In atypical AFl, re-entry may occur through any anatomical region in the left or right atrium.
- Atypical AFl is not classified according to the direction of impulse rotation.
- The diameter of re-entry in atypical AFl is at least 1 cm, corresponding to a re-entry path length of approximately 3 cm.
Unblocked AFl means that the AV node begins to conduct AFl impulses to the ventricles with 1:1 conduction (without block).
- The resulting ventricular rate is 240–300/min (the patient is hemodynamically unstable).
- Unblocked AFl may occur
- during treatment of AF with class IC antiarrhythmic drugs (Propafenone, Flecainide).
- Therefore, class IC antiarrhythmics are administered together with drugs that slow AV nodal conduction (beta-blockers, Verapamil, Diltiazem).
- The risk of unblocked AFl is 2–6 %
- in patients with AF or AFl receiving class IC antiarrhythmics without AV nodal blocking drugs,
- 20 % of patients with AF also have AFl, which may not be documented on ECG.
Mechanism of unblocked AFl during class IC antiarrhythmic therapy in patients with AFl:
- Class IC antiarrhythmics slow conduction within the re-entry circuit.
- An impulse circulating at approximately 300/min is slowed to 200–240/min.
- The impulse thus circulates more slowly within the re-entry circuit and with each “turn” begins to conduct to the ventricles through the AV node,
- because impulses reach the AV node at a rate at which 1:1 conduction becomes possible.
- At higher rates, impulses encounter the effective refractory period of the AV node,
- and the AV node blocks conduction, for example with 2:1 or 3:1 conduction.
When treating AF or AFl with class IC antiarrhythmics, AV nodal blocking drugs must always be co-administered:
- Beta-blockers, Verapamil, or Diltiazem,
- AV nodal blocking drugs prevent the occurrence of unblocked 1:1 AFl.
For treatment of AFl, radiofrequency ablation is recommended because antiarrhythmic therapy has minimal effect.
- The principle of pharmacological treatment of AFl is to slow conduction of AFl through the AV node,
- so that AFl is conducted to the ventricles at a rate of <100/min.
- AV nodal blocking drugs are used: beta-blockers, Verapamil, Diltiazem.
- Pharmacological therapy usually cannot terminate the re-entry circuit.
- Class IC antiarrhythmics slow re-entry but do not terminate it; there is a risk of unblocked 1:1 AFl,
- therefore class IC antiarrhythmics are always administered together with AV nodal blocking drugs:
- beta-blockers, Verapamil, Diltiazem.
| Atrial Flutter and Atrial Fibrillation |
Class |
| Anticoagulation therapy in atrial flutter is indicated according to the CHA2DS2-VA score. |
I |
| For treatment of atrial flutter, radiofrequency ablation is recommended. |
I |
When treating atrial fibrillation with class IC antiarrhythmics (Propafenone, Flecainide), it is recommended to also administer
- AV nodal blocking drugs (beta-blockers, Verapamil, or Diltiazem),
- to prevent unblocked 1:1 atrial flutter
- (20 % of patients with atrial fibrillation also have atrial flutter).
|
I |