
The vagus nerve innervates the following cardiac structures and causes:
The vagus nerve innervates the atria unevenly. Upon stimulation, uneven shortening of AP and ERP occurs, resulting in atrial dispersion (difference in duration) of AP and ERP, which creates a substrate for micro-reentry. This establishes a substrate for atrial fibrillation (AF).
Bradycardia prolongs atrial diastole, providing more time for the development of ectopic impulses and micro-reentry.
Vagal AF occurs due to parasympathetic (vagus nerve) stimulation.
The trigger of vagal AF is bradycardia.

| Vagal atrial fibrillation – most common triggers |
|---|
| Sleep |
| Postprandial state (after a large meal) |
| Relaxation after stress or after exercise |
| Alcohol (especially beer) |
| Nausea |
| Vomiting, swallowing |
AF may occur during sleep due to sleep apnoea syndrome (this does not have to be vagus-mediated).
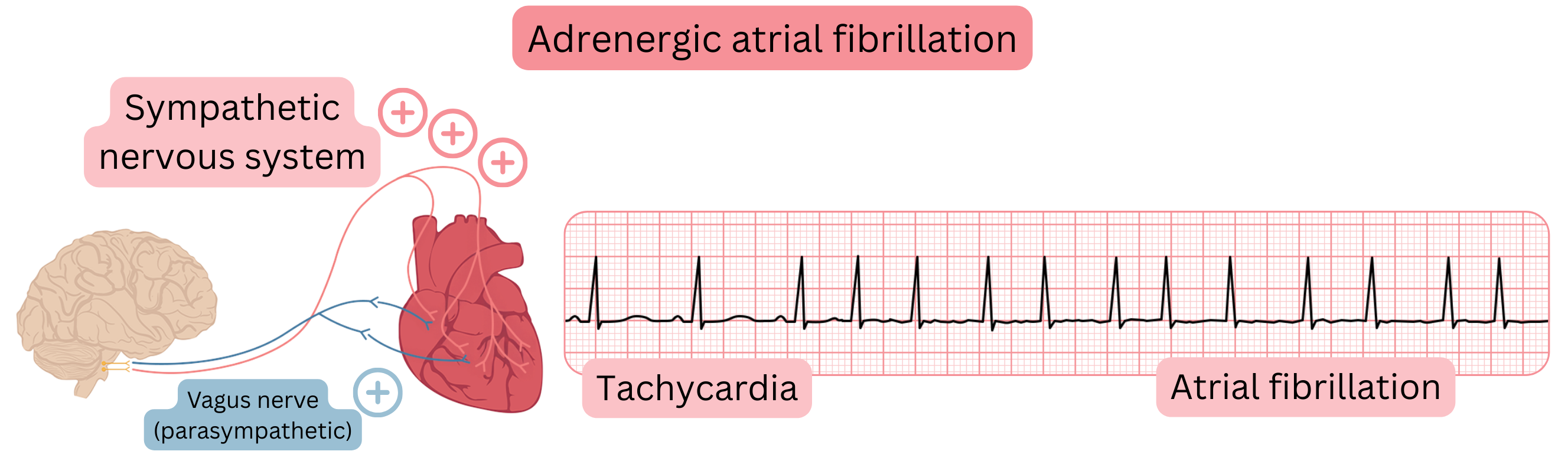
Adrenergic AF

Vagal AF
Athletes and vagal AF
| Vagal vs Adrenergic Atrial Fibrillation | |
|---|---|
| Vagal AF | Adrenergic AF |
| More common in younger patients (25–60 years) | More common in older patients (>60 years) |
| More common in men than women (4:1) | More common in men than women (2:1) |
| Without structural heart disease | Structural heart disease |
Induced by parasympathetic stimulation:
|
Induced by sympathetic stimulation:
|
| Occurs mainly at night | Occurs mainly during the day |
| Preceded by bradycardia | Preceded by tachycardia |
| Slow ventricular response (<100/min.) | Rapid ventricular response (>100/min.) |
| Worsens after beta-blocker administration | Improves after beta-blocker administration |
| Less frequently progresses to persistent AF | More frequently progresses to persistent AF |
For chronic treatment of vagal AF, the following is recommended:
For acute treatment of vagal AF (if the patient is not taking disopyramide), the following is recommended:
In vagal AF, bradycardia-inducing drugs should not be administered long-term:
In vagal AF, the primary issue is not AV nodal conduction itself, but marked vagal predominance in the atria, which triggers AF:
A single low dose of a beta-blocker or verapamil/diltiazem before flecainide in vagal AF:
| Vagal atrial fibrillation | Class |
|---|---|
| For long-term treatment of vagal atrial fibrillation, disopyramide is recommended. | I |
| For acute treatment of vagal AF (if the patient is not taking disopyramide), the “pill-in-the-pocket” strategy with flecainide is recommended. 30 minutes before flecainide, an AV node–slowing drug (beta-blocker, verapamil, diltiazem) is recommended as prevention of 1:1 atrial flutter conduction. | I |
In the treatment of vagal atrial fibrillation, the following antiarrhythmic drugs may be considered:
|
IIb |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
