
Rate control (control of the ventricular response) is a secondary treatment strategy in atrial fibrillation (AF).

The target ventricular rate (QRS) during long-term rate control of AF should be:
The rate control strategy in AF includes:
If a patient is diagnosed with AF, anticoagulation therapy is indicated according to the CHA2DS2-VA score
| Rate control of atrial fibrillation | Class |
|---|---|
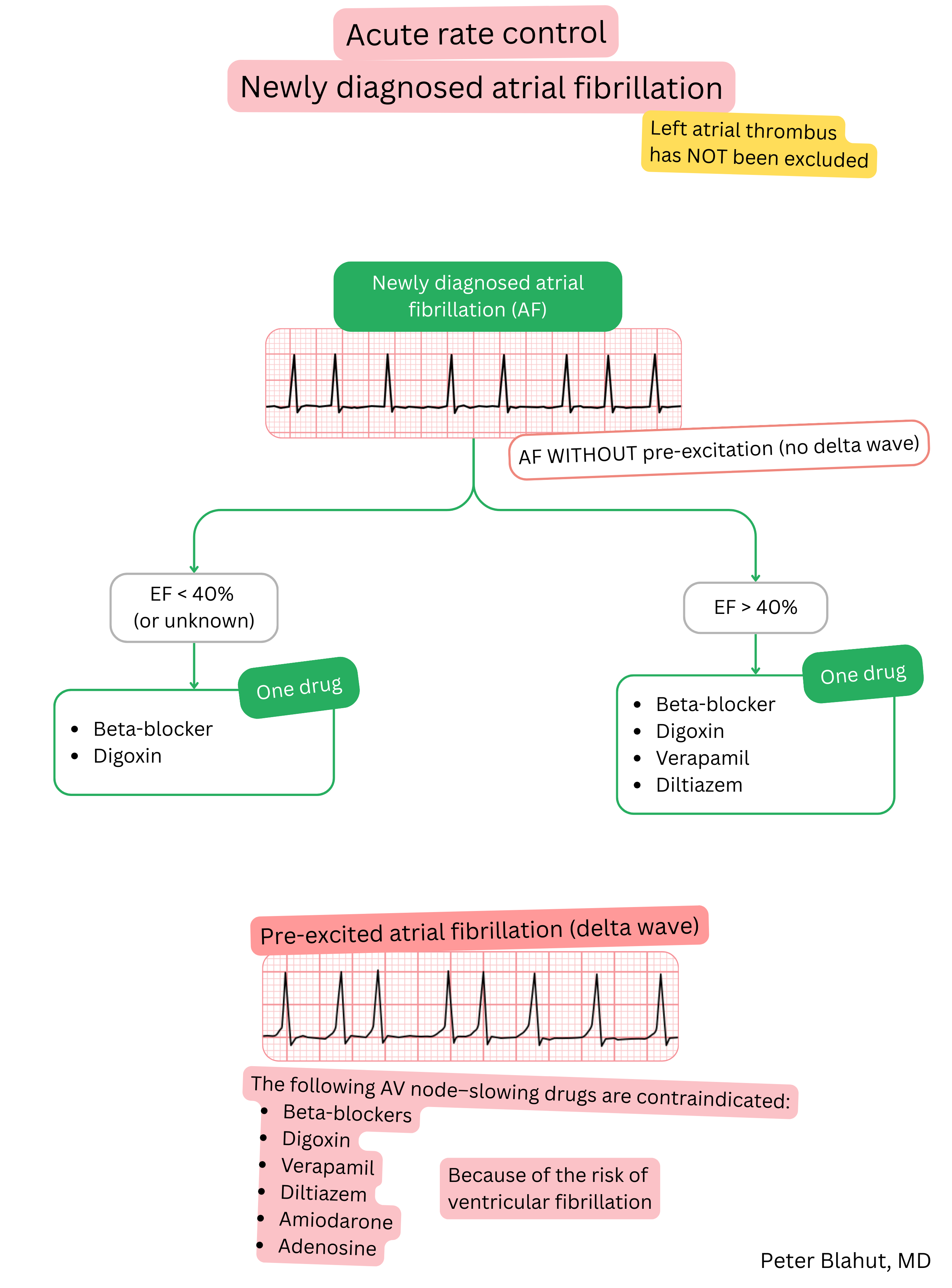
| Acute rate control in AF is recommended in every haemodynamically stable patient with newly diagnosed AF in whom left atrial thrombus has not been excluded. | I |
In pre-excited AF, drugs that slow AV nodal conduction are contraindicated:
|
III |
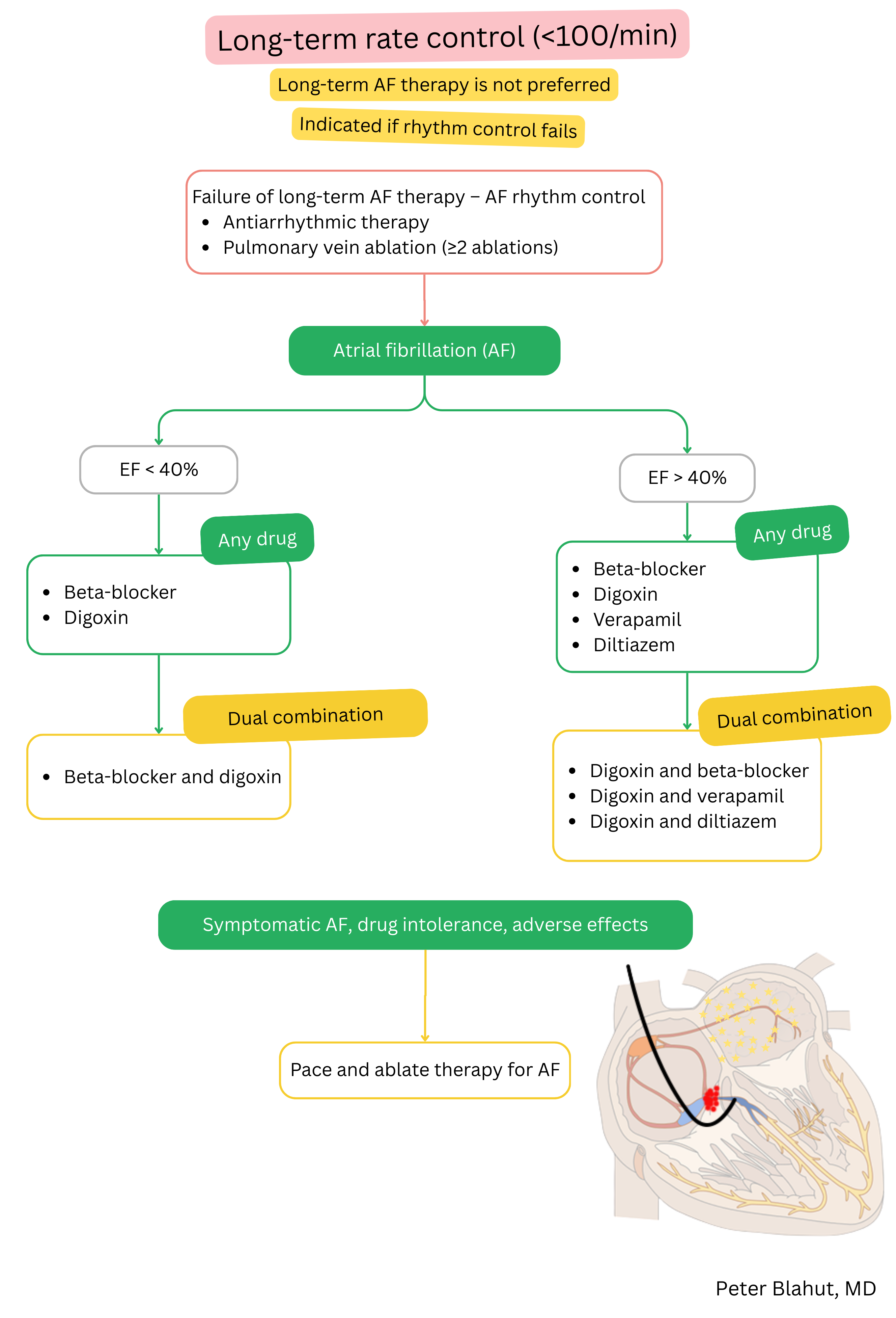
For rate control (acute or chronic) in a patient with AF and EF <40% the following are recommended:
|
I |
For rate control (acute or chronic) in a patient with AF and EF >40% the following are recommended:
|
I |
| Combination therapy for rate control should be considered if the effect of a single drug is inadequate. | IIa |
The target rate during long-term rate control of AF should be:
|
IIa |
Pace-and-ablate strategy (AV node ablation + pacemaker) should be considered if AF is symptomatic and there has been failure of:
|
IIa |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
