
The Pill in the Pocket strategy is acute termination of a paroxysmal atrial fibrillation (AF) episode in the home setting.

In the Pill in the Pocket strategy, Class IC antiarrhythmic drugs (propafenone, flecainide) are administered,
The Pill in the Pocket strategy is intended for patients without frequent episodes of paroxysmal AF and
Indications (Pill in the Pocket):
The patient receives chronic anticoagulation according to the CHA2DS2-VA score.

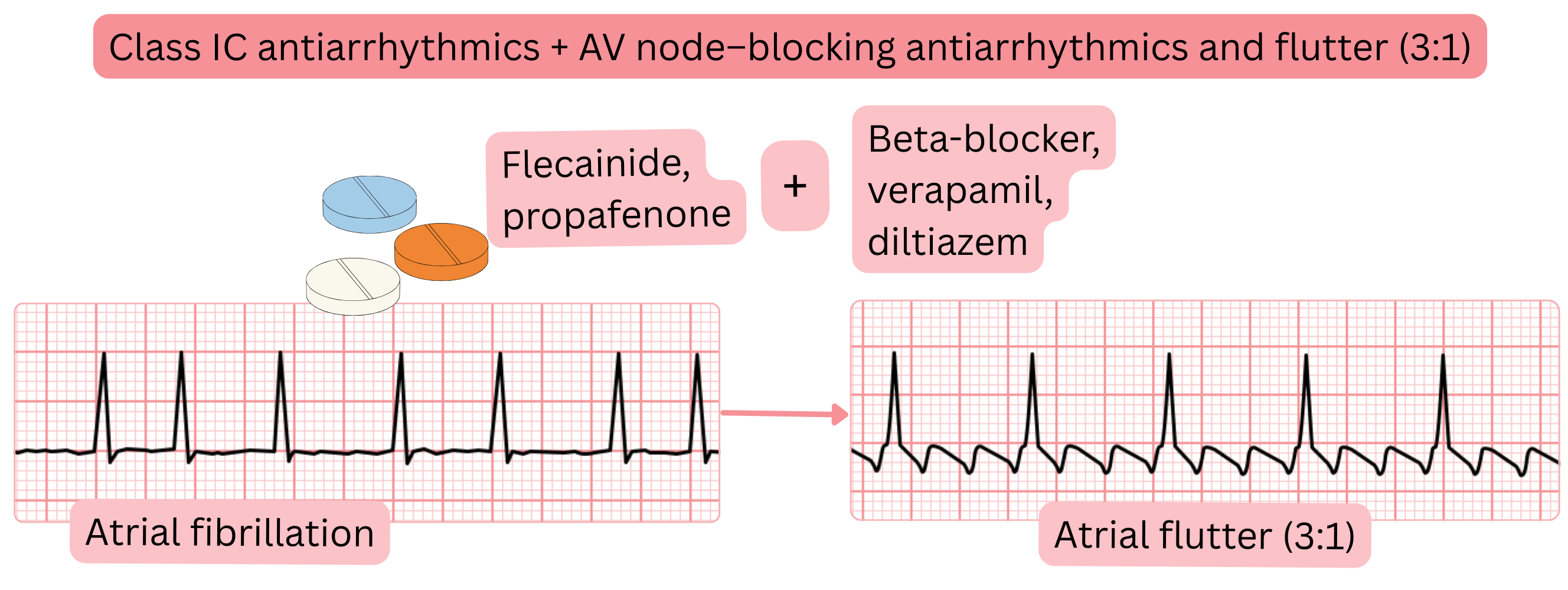
Class IC antiarrhythmic drugs and 1:1 conducted atrial flutter
| Prevention of 1:1 conducted atrial flutter before oral Class IC administration (propafenone, flecainide) | |||
|---|---|---|---|
| Drug | Route | Dose | Timing before Class IC administration |
| Metoprolol | oral | 25 mg | 30 min before Class IC administration |
| Verapamil | oral | 80 mg | 30 min before Class IC administration |
| Diltiazem | oral | 60 mg | 30 min before Class IC administration |
Pill in the Pocket treatment strategy:
| Pill in the Pocket – Class IC antiarrhythmic drugs | |||
|---|---|---|---|
| Drug | Route | Patient weight | Dose |
|
Flecainide (may be administered during pregnancy) |
oral | > 70 kg | 300 mg |
|
Flecainide (may be administered during pregnancy) |
oral | < 70 kg | 200 mg |
| Propafenone | oral | > 70 kg | 600 mg |
| Propafenone | oral | < 70 kg | 450 mg |
The patient may take the above single dose of a Class IC antiarrhythmic drug only once within 24 hours.
If cardioversion does not occur within 6 hours after taking the Class IC antiarrhythmic drug, the patient should seek medical attention.
| Class IC antiarrhythmic drugs (oral) – time to conversion and success rate | ||||
|---|---|---|---|---|
| Antiarrhythmic drug | Class | Time to conversion | Success rate | Typical patient |
| Flecainide (oral) | IC | 3–8 h | 50–85 % | Patient without structural heart disease. |
| Propafenone (oral) | IC | 3–8 h | 45–78 % | Patient without structural heart disease. |
| Pharmacological (oral) cardioversion of atrial fibrillation | Class |
|---|---|
| The “Pill in the Pocket” strategy (use of propafenone or flecainide at home) may be considered in patients with paroxysmal, oligosymptomatic atrial fibrillation with episodes occurring approximately once every 2–6 months. | IIa |
| In the “Pill in the Pocket” strategy (propafenone or flecainide), concomitant AV nodal–blocking therapy (beta-blocker, verapamil, diltiazem) should be used to prevent 1:1 conducted atrial flutter. | IIa |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
