
The substrate (trigger and substrate) for atrial fibrillation (AF) develops when an electrical disorder of the atria occurs as a result of atrial remodelling (structural, mechanical, or electrical). Atrial remodelling may be:
Acute atrial remodelling
Chronic atrial remodelling
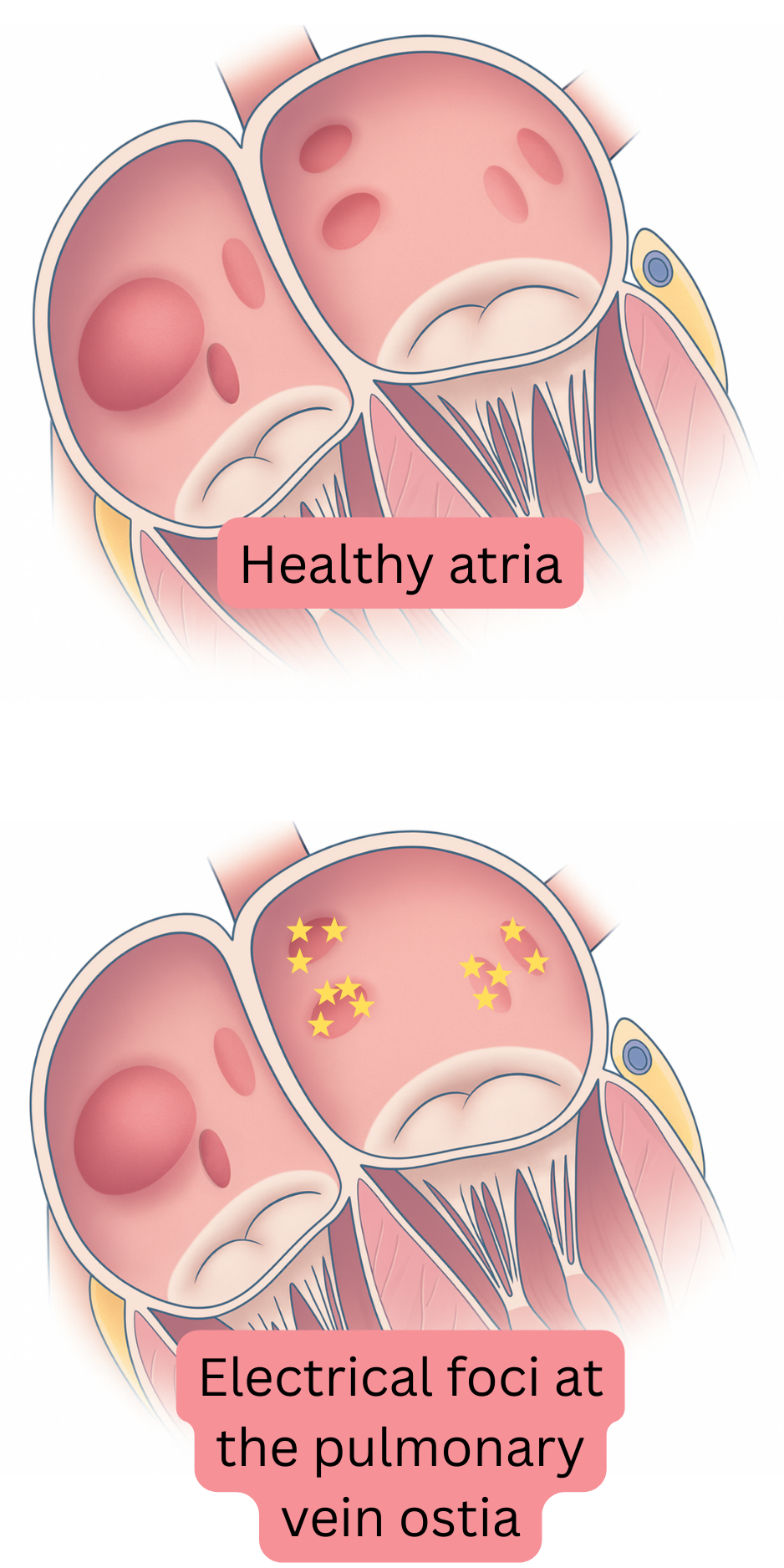
Atrial remodelling leads to the development of a trigger in the atria, with multiple electrical foci (5–20) generating impulses independently and activating the substrate. The resulting impulse rate is 300–600/min. The atria no longer produce synchronous systole but instead fibrillate—“quiver”.
Remodelling most commonly begins in the region of the pulmonary vein ostia in the left atrium, where both the trigger and substrate for AF gradually develop. The ostium is the anatomical region where the pulmonary vein connects to the left atrium. Remodelling then progressively extends to the entire left atrium and partially to the right atrium over 5–15 years.
| Pathophysiology of atrial fibrillation |
|---|
| The substrate (trigger and substrate) for atrial fibrillation most commonly develops due to atrial cardiomyopathy. |
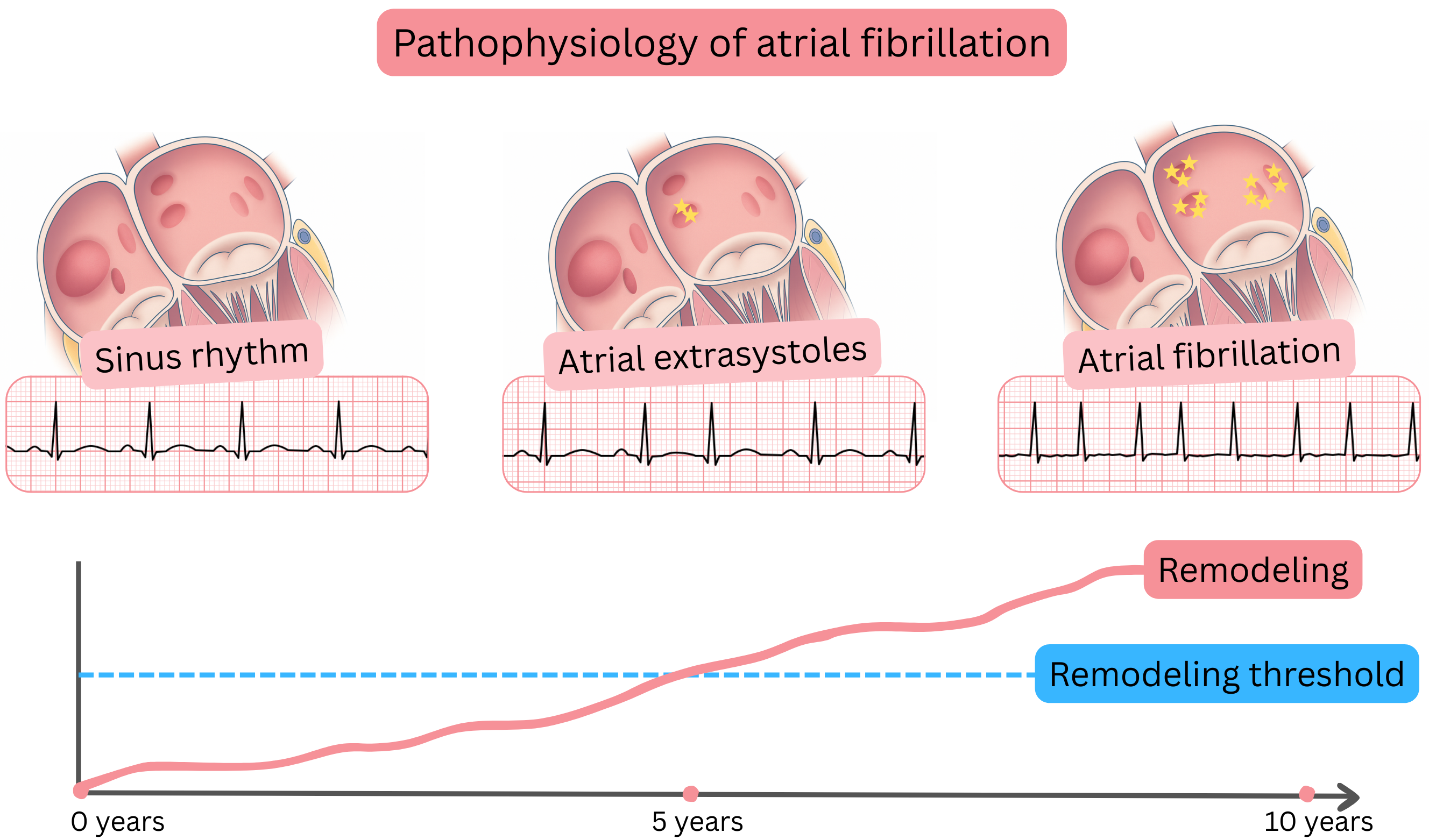
| The pre-fibrillatory state consists of premature atrial contractions or atrial tachycardia originating from the region of the pulmonary vein ostia, which may sometimes be visible on the ECG. |
| The pre-fibrillatory state progresses within 6–12 months to paroxysmal atrial fibrillation. |
| Paroxysmal atrial fibrillation is most commonly triggered by premature atrial contractions or atrial tachycardia originating from the pulmonary vein ostia. |
The pulmonary vein ostia have different electrophysiological properties compared with the atrial myocardium. The ostia contain the highest density of autonomic nerve fibres and have a short refractory period. Therefore, even minimal remodelling in the ostial region readily leads to the development of foci (triggers) that generate impulses through triggered activity or abnormal automaticity. These foci then generate premature atrial contractions or atrial tachycardia, which activate the substrate and initiate AF.
Pre-fibrillatory state
Remodelling threshold
Trigger of atrial fibrillation
Episode of atrial fibrillation
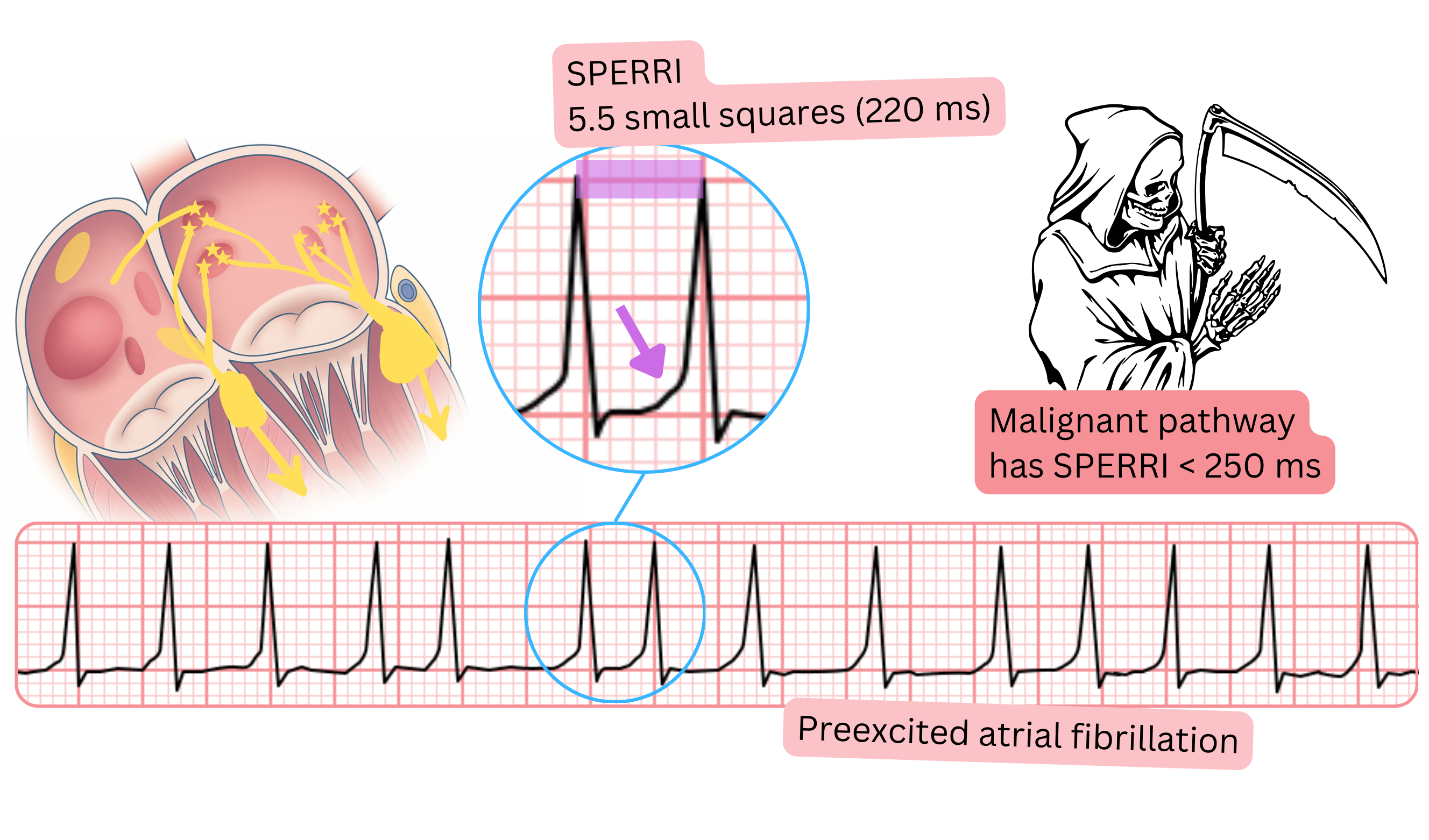
Pre-excited atrial fibrillation
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
