
According to the Vaughan Williams classification, antiarrhythmic drugs are divided into four main classes (I–IV).
Antiarrhythmic drugs are classified according to which receptors in the heart they act on:
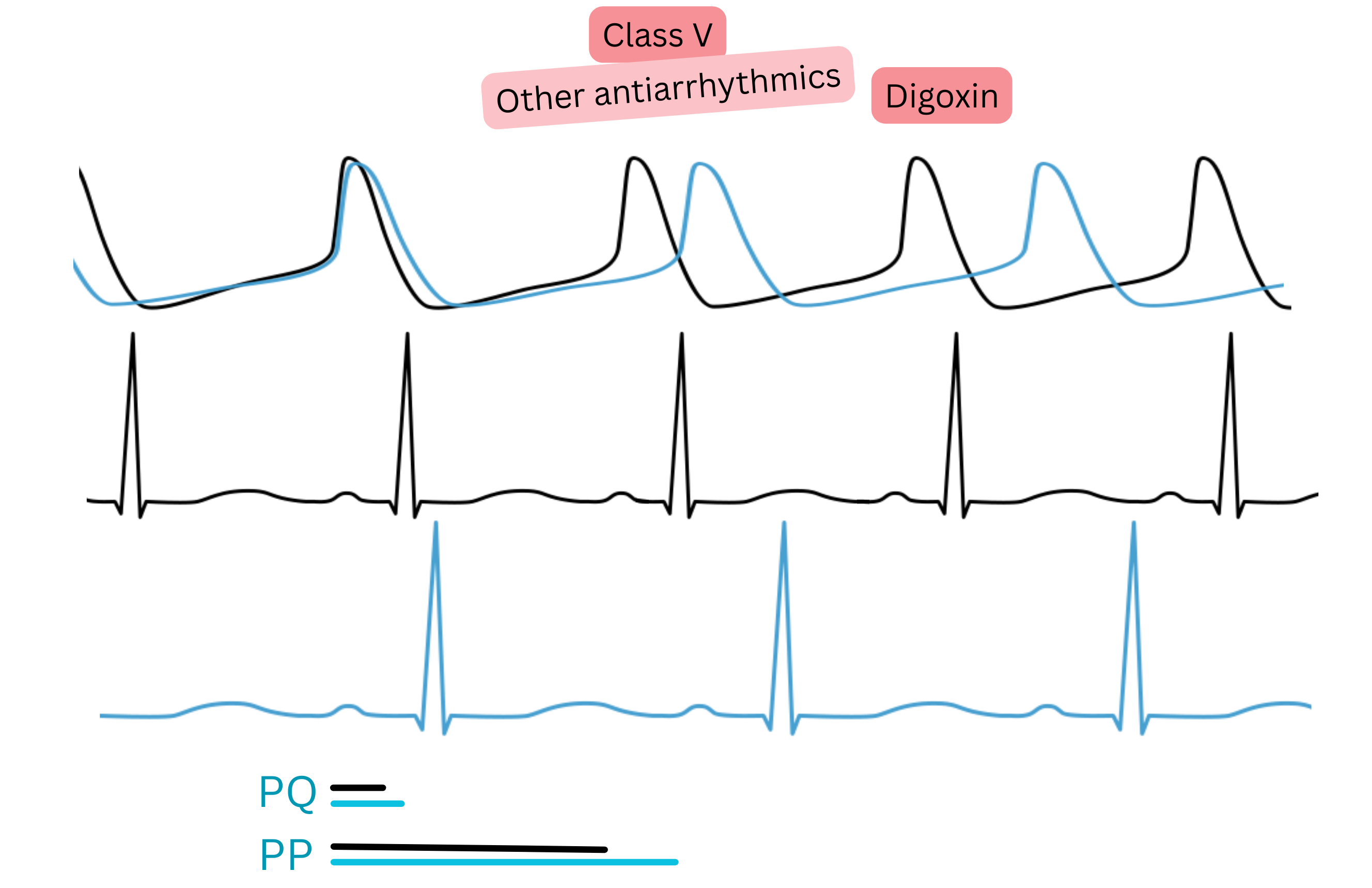
Digoxin is an antiarrhythmic drug, but it does not act directly on receptors in the heart.
| Vaughan Williams classification – antiarrhythmic drugs in atrial fibrillation (AF) | |||||
|---|---|---|---|---|---|
| Class | Mechanism | ECG effect | Antiarrhythmic drug | Main use in AF | Note |
| I A | Na⁺ blockade + mild K⁺ blockade | ↑ QT, ± ↑ QRS |
Procainamide | Cardioversion (acute intravenous) | Risk of TdP with prolonged QT |
| Disopyramide | Rhythm control (rarely) | Anticholinergic adverse effects (urinary retention, glaucoma) | |||
| I C | Strong Na⁺ blockade | ↑ QRS | Flecainide | Cardioversion, rhythm control | Only in the absence of structural heart disease (CAST trial) |
| Propafenone | Cardioversion, rhythm control | Only in the absence of structural heart disease (CAST trial) | |||
| II | β-receptor blockade | ↑ PR, ↓ rate |
Beta-blockers | Rate control | First choice in AF + hypertension/ischaemic heart disease |
| III | K⁺ channel blockade (some also Na⁺, Ca²⁺, β-blockade) | ↑ QT, ± ↑ QRS/PR |
Amiodarone | Cardioversion, rhythm control | Most effective, but many adverse effects with long-term use |
| Sotalol | Rhythm control | Requires QTc monitoring, risk of TdP | |||
| Dronedarone | Rhythm control (less effective) | A “weak amiodarone” | |||
| Ibutilide | Cardioversion (intravenous) | Acute cardioversion of pre-excited AF and atrial flutter, risk of TdP | |||
| IV | Ca²⁺ channel blockade (non-DHP) | ↑ PR, ↓ rate |
Verapamil | Rate control | Contraindicated if EF < 40 % |
| Diltiazem | Rate control | Preferred in hypertension and AF | |||
| V | Various mechanisms | Various effects | Digoxin | Rate control | Effective at rest, less during exertion. Preferred if EF < 40 % |
| Vernakalant | Cardioversion (intravenous) | Atrial-selective, few adverse effects | |||
TdP – Torsades de Pointes, AFl – atrial flutter, IHD – ischaemic heart disease
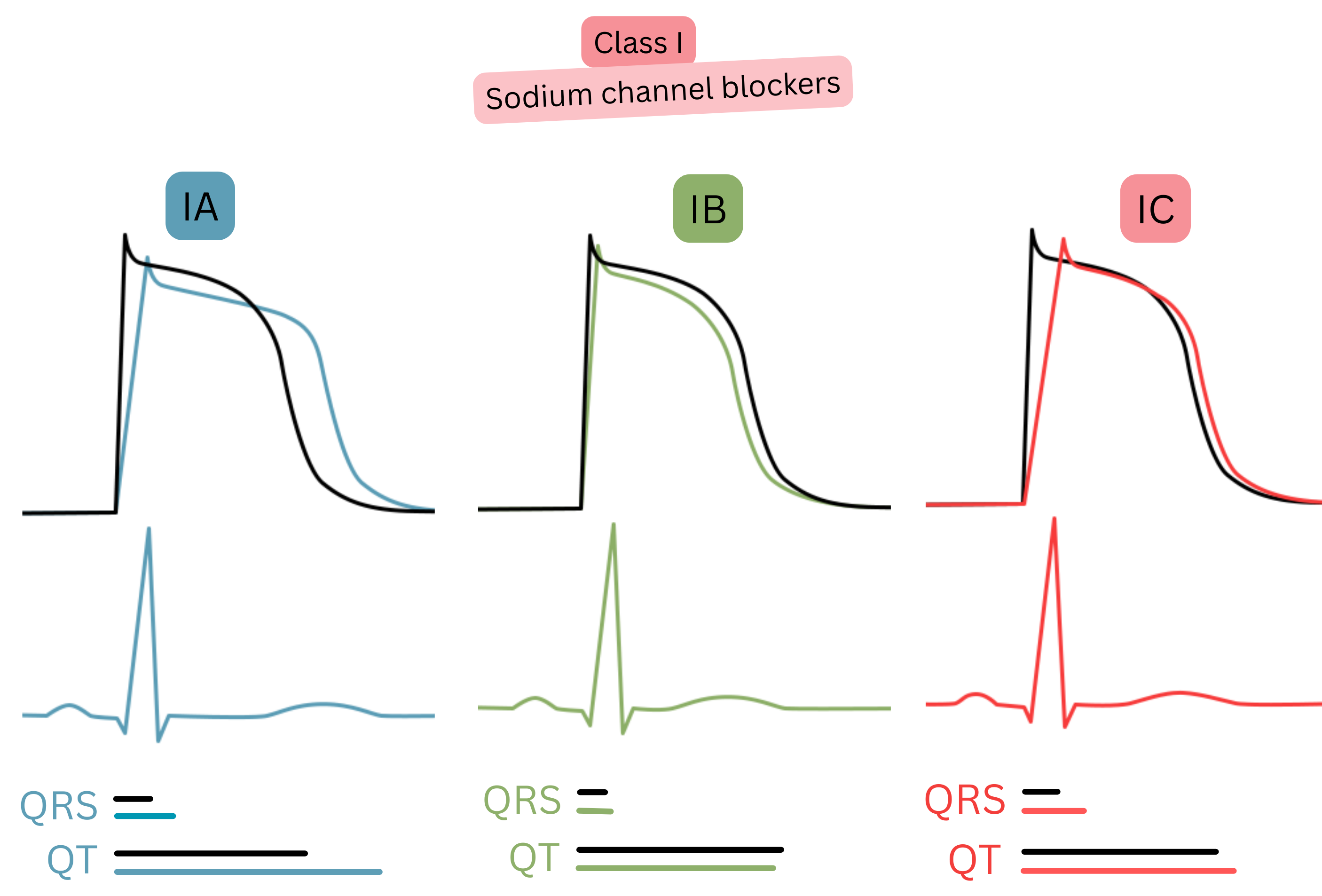
Class I (Na⁺ channel blockers)
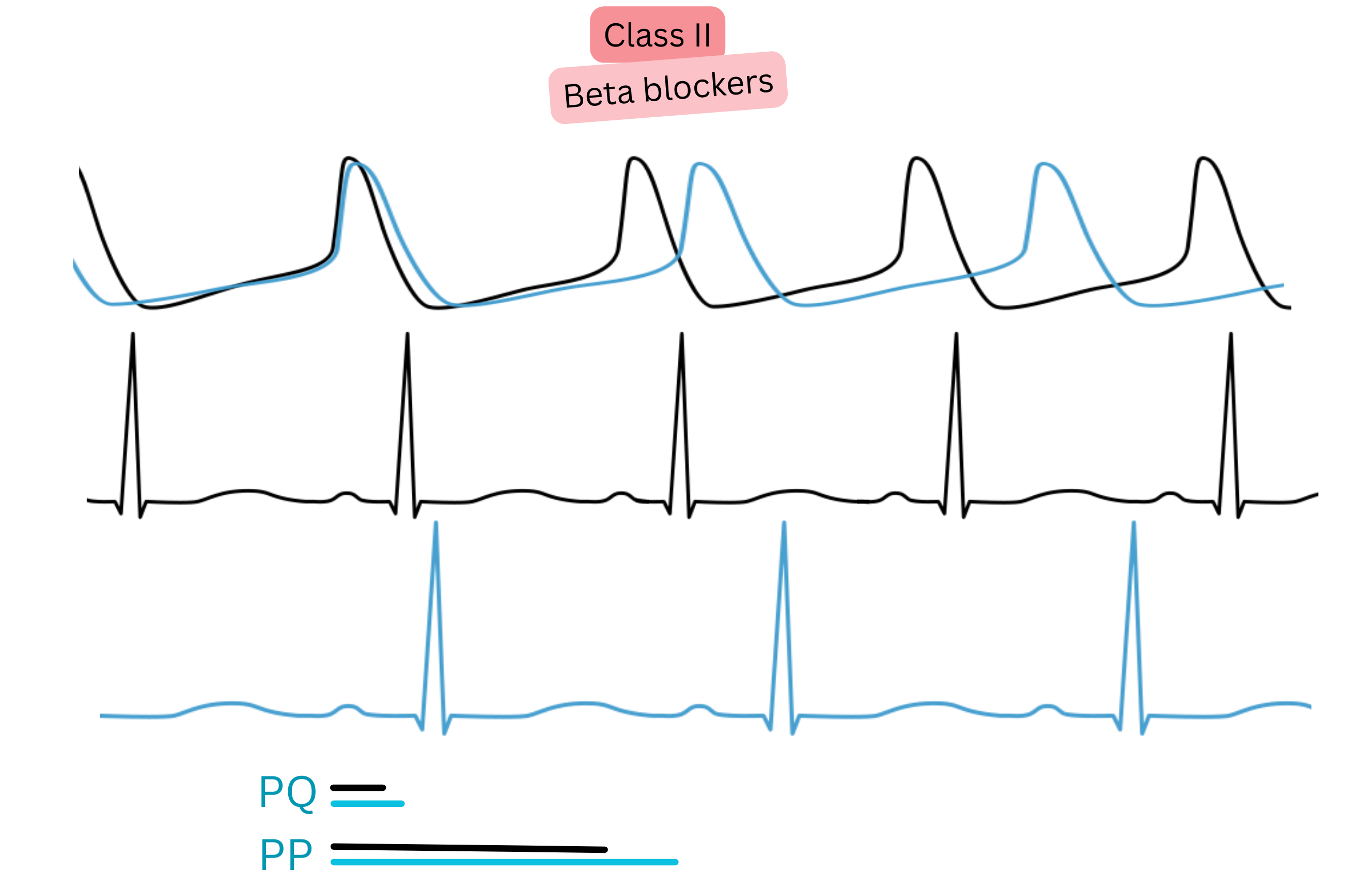
Class II (Beta-blockers)
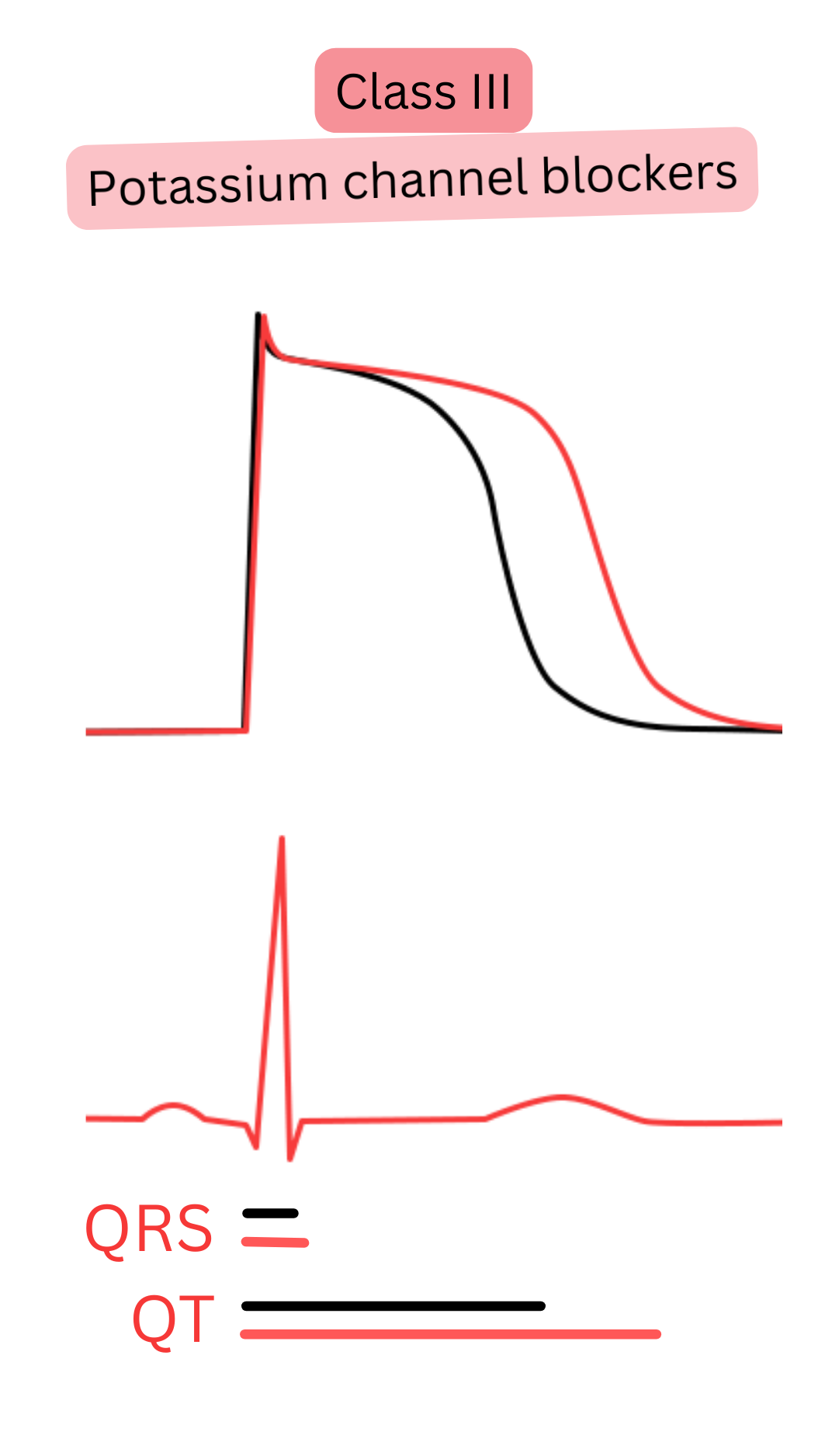
Class III (K⁺ channel blockers)
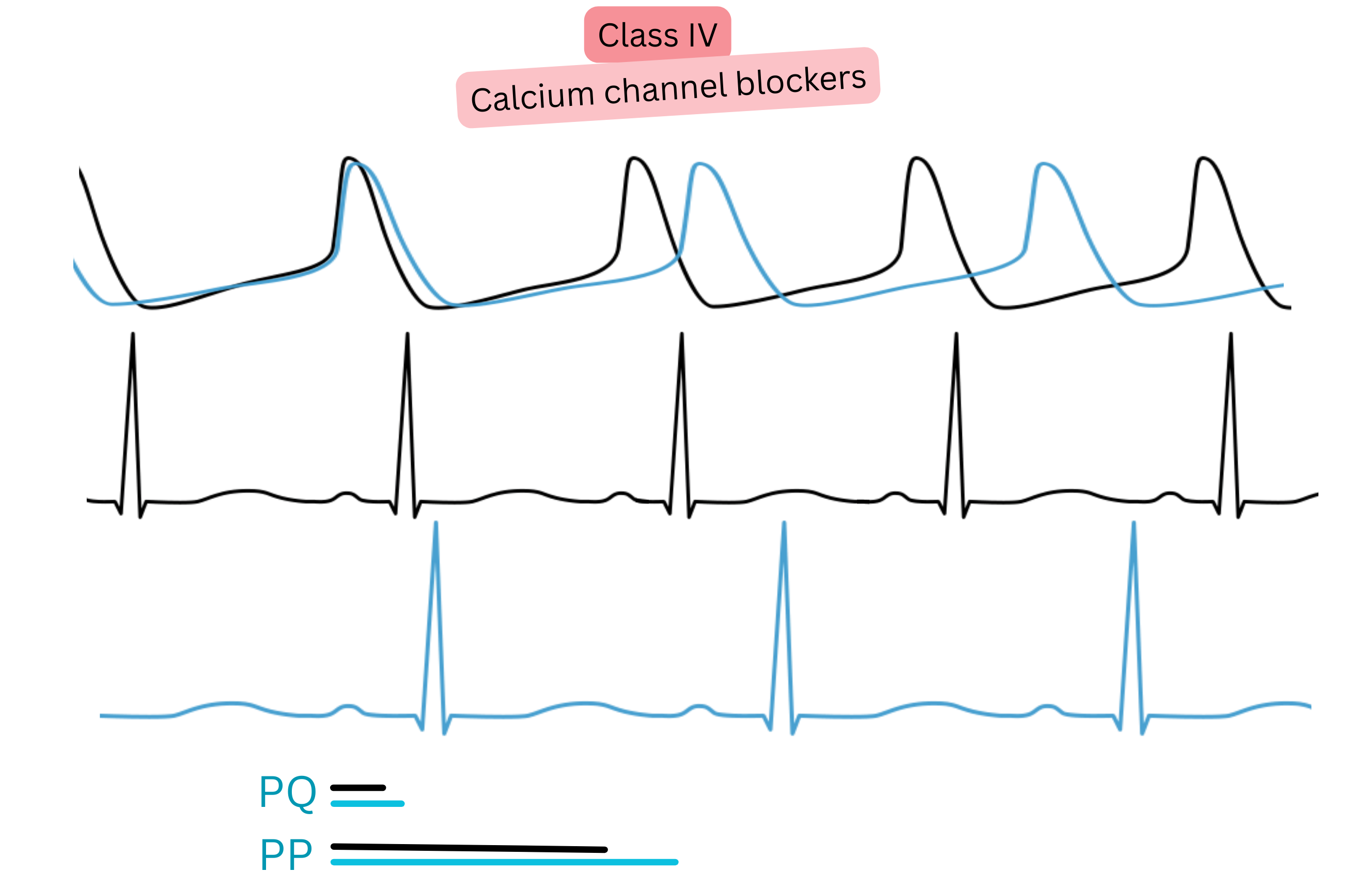
Class IV (Ca²⁺ channel blockers)
Digoxin
| Antiarrhythmic treatment – Main contraindications | Class |
|---|---|
Antiarrhythmic treatment is not recommended in patients:
|
III |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
