
Pharmacological (intravenous) cardioversion is used for acute cardioversion of atrial fibrillation (AF).
Indications for pharmacological (intravenous) cardioversion of AF:
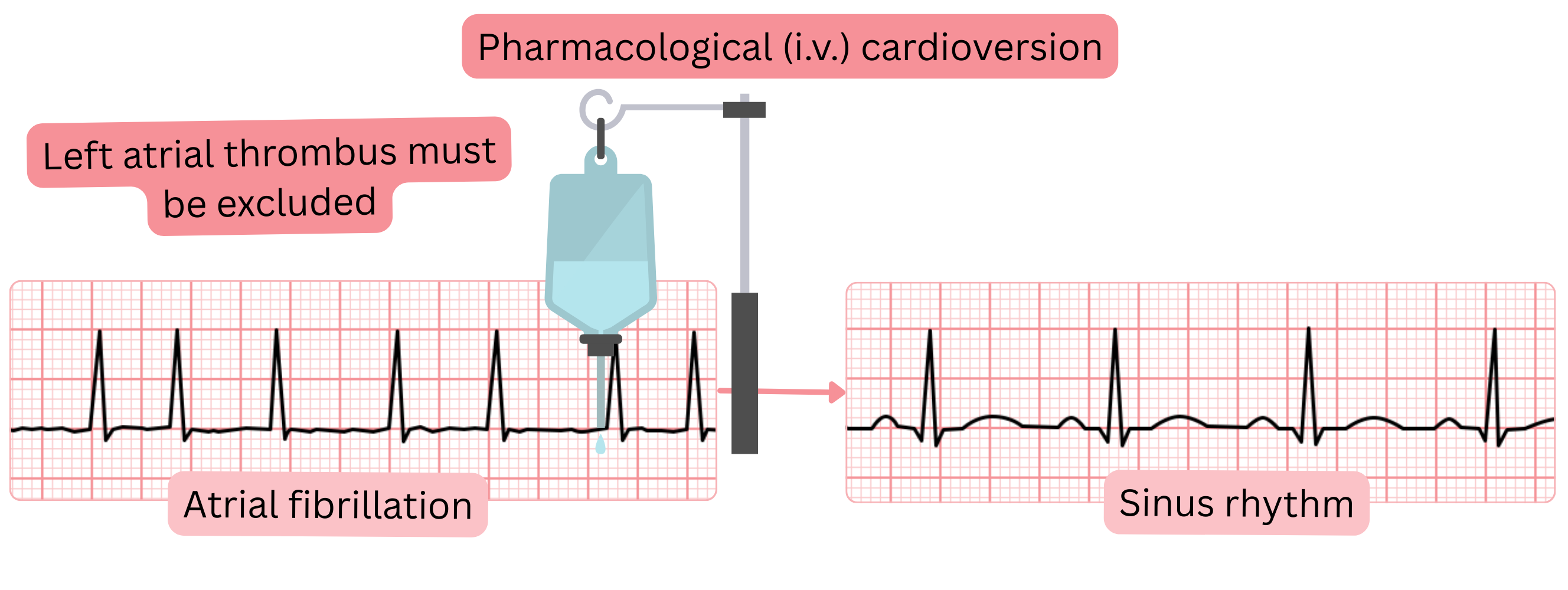
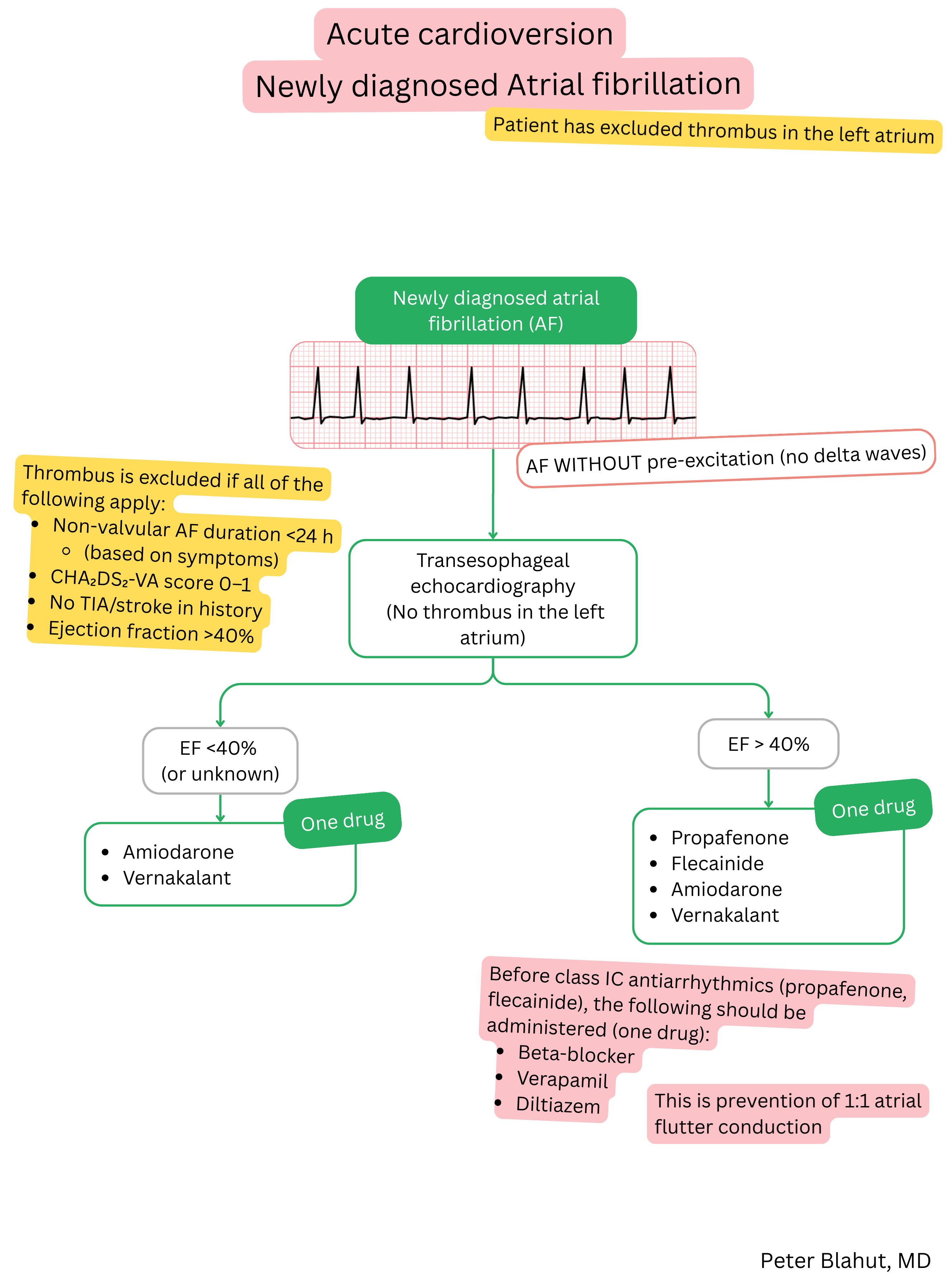
Before pharmacological (intravenous) cardioversion, left atrial thrombus must be excluded:
If the patient has a first-ever AF episode lasting <24 hours, cardioversion may be considered without thrombus exclusion.
Contraindications
Relative contraindications
Antiarrhythmic drugs used for (intravenous) cardioversion of AF:
| Antiarrhythmic drugs for cardioversion of atrial fibrillation (intravenous) | ||||
|---|---|---|---|---|
| Antiarrhythmic drug | Class | Time to conversion | Success rate | Typical patient |
| Propafenone | IC | < 6 h | 43–89 % | Patient without structural heart disease |
| Flecainide | IC | < 6 h | 52–95 % | Patient without structural heart disease |
| Amiodarone | III | 6–8 h | 44–80 % | Patient with structural heart disease / HFrEF |
| Vernakalant | III | < 10 min | 50–70 % | Recent-onset AF (< 7 days) |
| Ibutilide | III |
30–90 min (AF) < 60 min (atrial flutter) |
30–50 % (AF) 60–75 % (atrial flutter) |
AF or atrial flutter, including pre-excited AF |
| Procainamide | IA | < 30 min | 50–75 % | AF with pre-excitation |
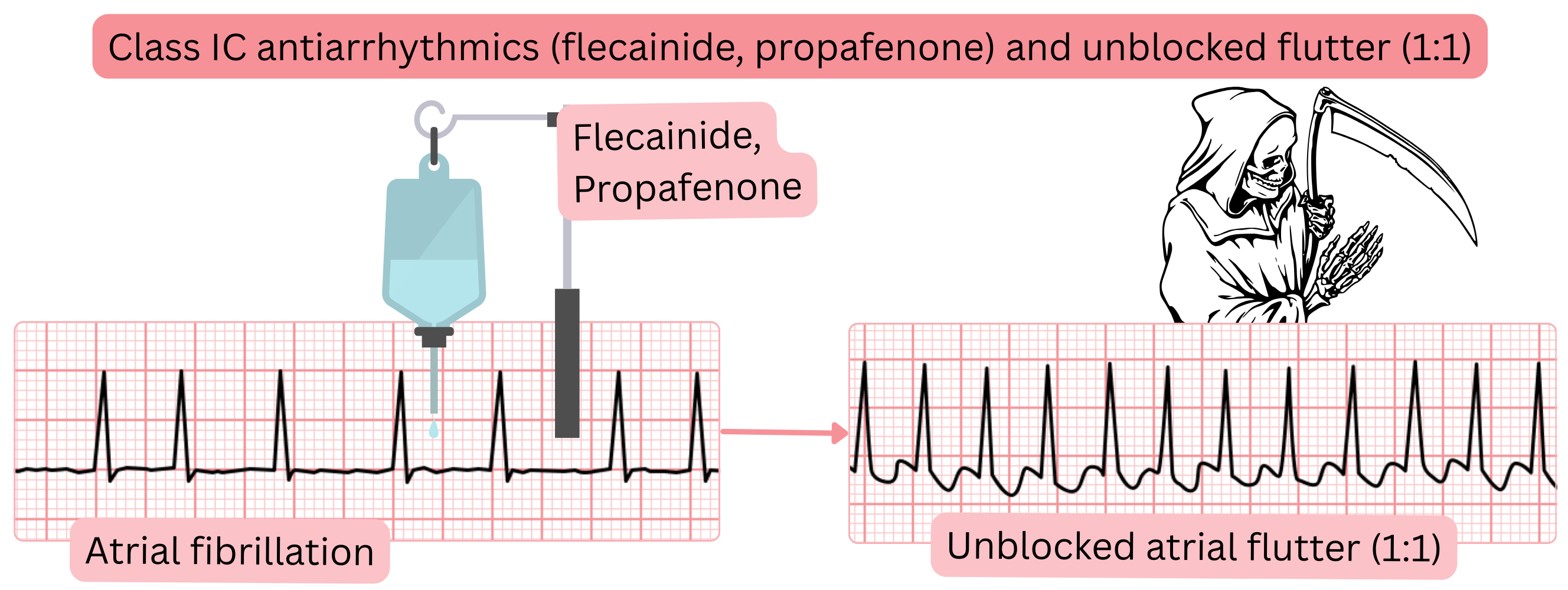
Class IC antiarrhythmic drugs and 1:1 conducted atrial flutter
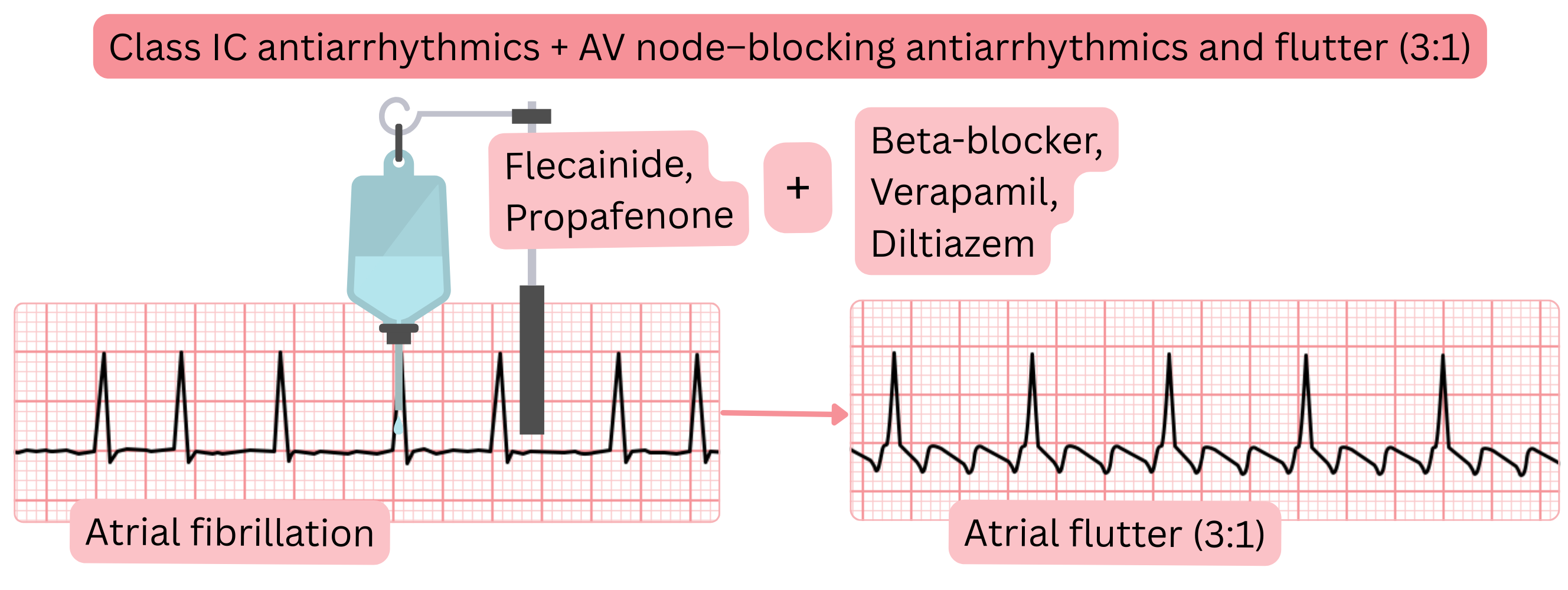
| Prevention of 1:1 conducted atrial flutter before Class IC administration (propafenone, flecainide) | |||
|---|---|---|---|
| Drug | Route | Dose | Timing before Class IC |
| Metoprolol | oral | 25 mg | 30 min before Class IC administration |
| Metoprolol | intravenous | 5 mg administered over 1–2 minutes | 20 min before Class IC administration |
| Verapamil | oral | 80 mg | 30 min before Class IC administration |
| Verapamil | intravenous | 5 mg administered over 1–2 minutes | 5 min before Class IC administration |
| Diltiazem | oral | 60 mg | 30 min before Class IC administration |
| Diltiazem | intravenous | 15 mg administered over 1–2 minutes | 5 min before Class IC administration |
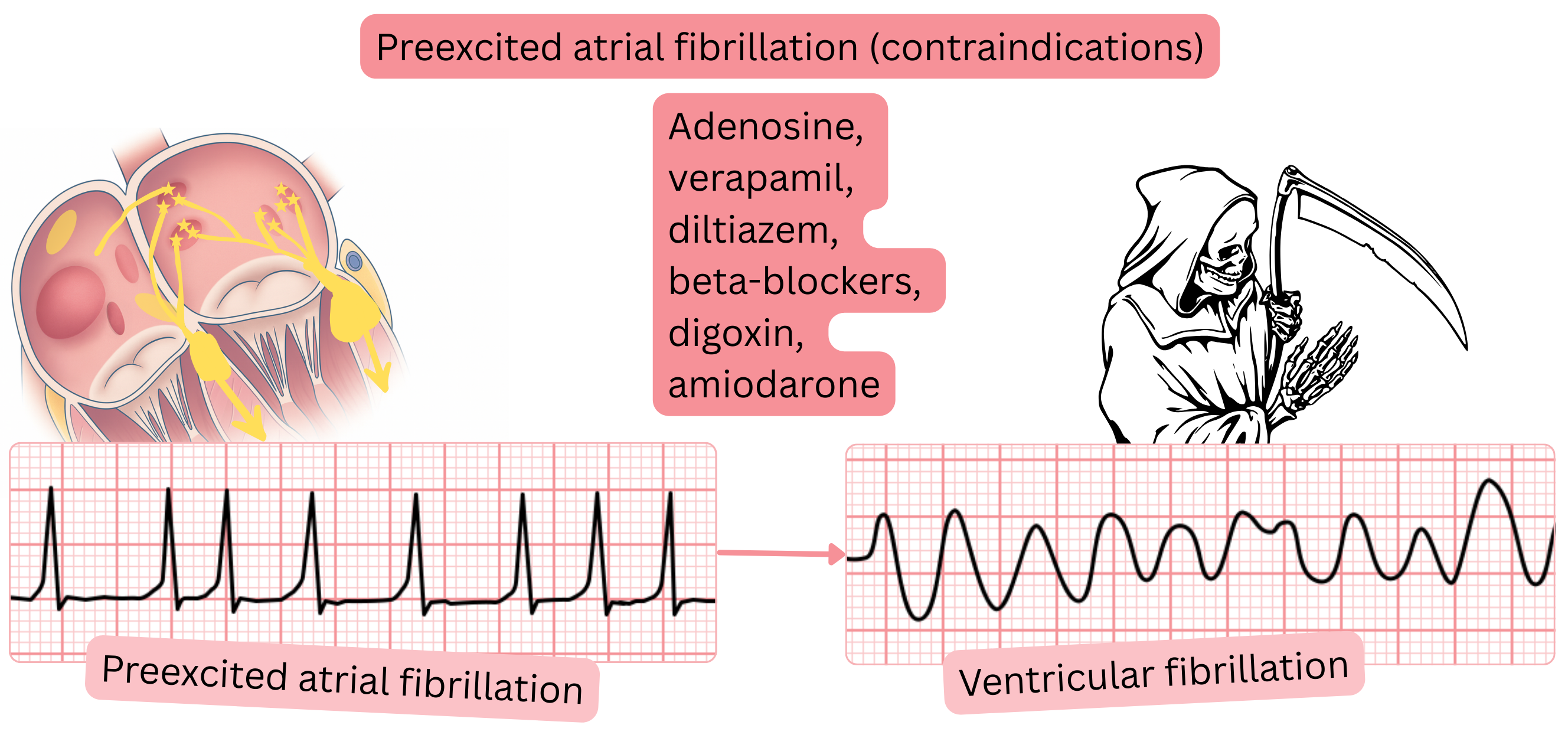
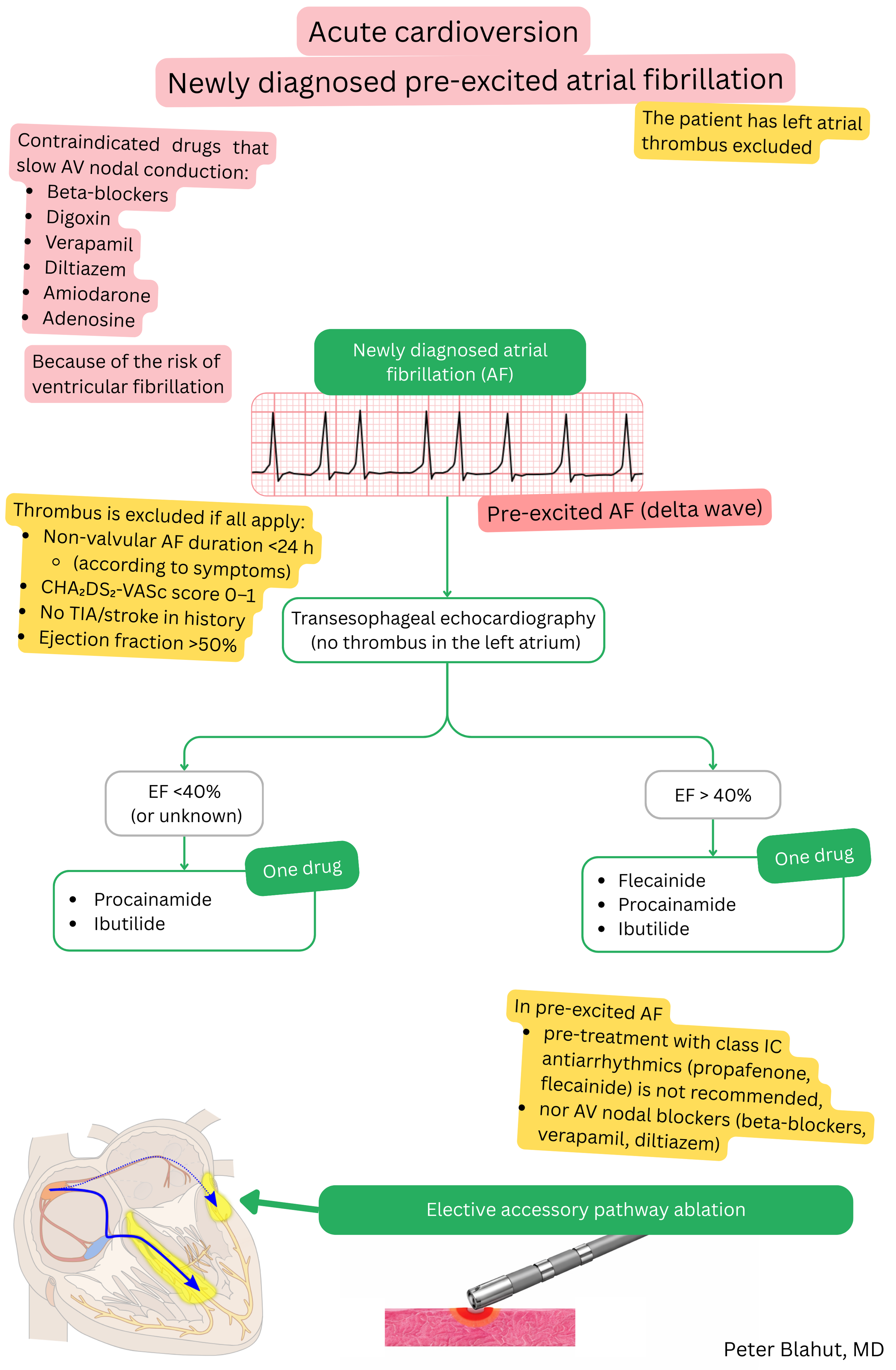
In pre-excited AF, antiarrhythmic drugs that prolong the effective refractory period (ERP) of the accessory pathway are recommended:
In pre-excited AF, antiarrhythmic drugs that slow AV nodal conduction are contraindicated.
| Contraindicated antiarrhythmic drugs – pre-excited atrial fibrillation | ||
|---|---|---|
| Drug | Class | Reason contraindicated |
| Verapamil, diltiazem | IV (Ca2+ channel blockers) | Slow only the AV node → increase conduction via the accessory pathway |
| Beta-blockers | II | Slow the AV node → risk of rapid 1:1 conduction over the accessory pathway |
| Digoxin | Inotropic agent, AV nodal blocker | Increases parasympathetic tone → AV nodal slowing, preferential accessory pathway conduction |
| Adenosine | AV nodal blocker | Blocks the AV node → allows rapid impulse conduction via the accessory pathway |
| Amiodarone (intravenous) | III | Unpredictable effect on the accessory pathway, risk of accelerated conduction |
Maintenance of sinus rhythm (SR) after cardioversion, despite antiarrhythmic therapy, is individual.
Atropine dosing for bradycardia after AF cardioversion:
| Pharmacological (intravenous) cardioversion of atrial fibrillation | Class |
|---|---|
Left atrial thrombus is considered excluded if all of the following criteria are met:
|
I |
| Flecainide or propafenone (intravenous) are recommended for pharmacological cardioversion of atrial fibrillation in patients without structural heart disease. | I |
| Before administration of Class IC antiarrhythmic drugs (flecainide, propafenone), AV nodal–blocking agents (beta-blocker, verapamil, diltiazem) should be administered to prevent 1:1 conducted atrial flutter. | IIa |
| Vernakalant (intravenous) is recommended for pharmacological cardioversion of atrial fibrillation in patients with EF >40%, without myocardial infarction within the last 30 days and without severe aortic stenosis. | I |
| Amiodarone (intravenous) is recommended for pharmacological cardioversion of atrial fibrillation in patients with structural heart disease. | I |
Pharmacological cardioversion is not recommended in patients (without a pacemaker) who have:
|
III |
In pre-excited AF, the following are contraindicated:
|
III |
These guidelines are unofficial and do not represent formal guidelines issued by any professional cardiology society. They are intended for educational and informational purposes only.
